
Abstract
Background
Although enhanced recovery after bariatric surgery (ERABS) has proven to be safe and cost-effective, this concept is relatively new in the Middle East.
Methods
A retrospective analysis of consecutive registered cohorts of patients who underwent primary and purely laparoscopic sleeve gastrectomy (LSG) or laparoscopic Roux-en-Y gastric bypass (LRYGB) were compared before introduction of ERABS (2010–2014) and after ERABS (2015–2017) at Tawam Hospital/Johns Hopkins, the UAE.
Results
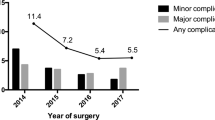
A total of 462 eligible bariatric patients (LSG 414 and LRYGB 48) were operated on before and 1602 (LSG 1436 and LRYGB 166) after introduction of the ERABS. Significant improvements of mean patient time of the patient being within the OR for LSG (from 2:27 to 1:23 min, p = 0.000) and LRYGB (from 3:17 to 1:59 min, p = 0.000) were achieved when comparing pre-ERABS with after introduction of ERABS. Furthermore, there was a significant decrease in LOS in both LSG (from 3.2 to 1.5 days, p = 0.000) and in LRYGB (from 3.5 to 1.7 days, p = 0.000). Major (CD classification III–IV) complications decreased significantly in LSG (from 13.8 to 0.8%, p = 0.000) and were similar in LRYGB (from 4.2% to 3.0%, p = NS). The readmission rate for LSG (from 2.9 to 2.6%, p = NS) or LRYGB (from 0 to 4.8%, p = NS) and the reoperation rates after LSG (from 0.7 to 0.5%, p = NS) and LRYGB (from 0 to 2.4%, p = NS) did not differ between both groups following introduction of ERABS.
Conclusions
Implementation of a standardized ERABS program in the Middle East is feasible and safe and leads to reduced LOS and OR times.

Similar content being viewed by others


References
Alshaikh MK, Filippidis FT, Al-Omar HA, et al. The ticking time bomb in lifestyle-related disease among women in the Gulf Cooperation Council countries: a review of systematic reviews. BMC Public Health. 2017;17:536.
Alhyas L, McKay A, Balasanthiran A, et al. Prevalences of overweight, obesity, hyperglycemia, hypertension and dyslipidaemia in the Gulf: a systematic review. JRSM Short Rep. 2011;2:55.
Anselmino M, Bammer T, Fernandez Cebrian JM, et al. Cost-effectiveness and budget impact of obesity surgery in patients with type 2 diabetes in three European countries. Obes Surg. 2009;19:1542–9.
Mullen DM, Marr TJ. Longitudinal cost experience for gastric bypass patients. Surg Obes Relat Dis. 2010;6:243–8.
Powers KA, Rehrig ST, Jones DB. Financial impact of obesity and bariatric surgery. Med Clin North Am. 2007;91:321–38.
Keating CL, Dixon JB, Moodie ML, et al. Cost-effectiveness of surgically induced weight loss for the management of type 2 diabetes: modeled lifetime analysis. Diabetes Care. 2009;32:567–74.
Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg. 2008;248:189–98.
Birkmeyer JD, Dimick JB, Staiger DO. Operative mortality and procedure volume as predictors of subsequent hospital performance. Ann Surg. 2006;243:411–7.
Main DS, Henderson WG, Pratte K, et al. Relationship of processes and structures of care in general surgery to postoperative outcomes: a descriptive analysis. J Am Coll Surg. 2007;204:1157–65.
Chowdhury MM, Dagash H, Pierro A. A systematic review of the impact of volume of surgery and specialization on patient outcome. Br J Surg. 2007;94:145–61.
Campillo-Sota A et al. Evaluation of the clinical pathway for laparoscopic bariatric surgery. Obes Surg. 2008;18:395–400.
Cooney RN, Bryant P, Haluck R, et al. The impact of a clinical pathway for gastric bypass surgery on resource utilization. J Surg Res. 2001;98:97–101.
Mannaerts GH, van Mil SR, Stepaniak PS, et al. Results of implementing an enhanced recovery after bariatric surgery (ERABS) protocol. Obes Surg. 2016;26:303–12.
Fried M, Yumuk V, Oppert J-M, et al. Inter-disciplinary European guidelines on metabolic and bariatric surgery. Obes Facts. 2013;6:449–68.
Gadiot RP, Biter LU, Zengerink HJ, et al. Laparoscopic sleeve gastrectomy with an extensive posterior mobilization: technique and preliminary results. Obes Surg. 2012;22:320–9.
Jacobsen HJ, Bergland A, Raeder J, et al. High-volume bariatric surgery in a single center: safety, quality, cost-efficacy and teaching aspects in 2,000 consecutive cases. Obes Surg. 2012;22:158–66.
Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250:187–96.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications. Ann Surg. 2014;240:205–13.
Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systemic analysis for the Global Burden Disease Study. Lancet 2013. 2013;384:766–81.
Driscoll S, Gregory DM, Fardy JM, et al. Long-term health-related quality of life in bariatric surgery patients: a systematic review and meta-analysis. Obesity. 2016;24:60–70.
Yu J, Zhou X, Li L, et al. The long-term effects of bariatric surgery for type 2 diabetes: systematic review and meta-analysis of randomized and non-randomized evidence. Obes Surg. 2015;25:143–58.
Picot J, Jones J, Jl C, et al. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Health Technol Assess. 2009;13:1–190.
Malczak P, Pisarska M, Piotr M, et al. Enhanced recovery after bariatric surgery: systematic review and meta-analysis. Obes Surg. 2017;27:226–35.
Mil V, Duinhouwer LE, Mannaerts GH, et al. The standardized postoperative checklist for bariatric surgery; a tool for safe early discharge. Obes Surg. 2017;27:3102–9.
Sippey M, Karsten KR, Chapman WH, et al. 30-day readmissions after sleeve gastrectomy versus bypass. Surg Obes Relat Dis. 2016;12:991–6.
Loots E, Sartorius B, Paruk IM, et al. The successful implementation of a modified enhanced recovery after surgery program for bariatric surgery in a South African teaching hospital. Surg Laparosc Endosc Percutan Tech. 2018;28:26–9.
May C, Finch T. Implementation embedding and integrating practices: an outline of normalisation process theory. Sociology. 2009;43:535–54.
Sutton E, Herbert G, Burden S, et al. Using the normalization process theory to qualitatively explore sense-making in implementation of the enhanced recovery after surgery programme: “It’s not rocket science”. PLoS One. 2018;13:e0195890.
Stepaniak PS, Mannaerts GH, de Quelerij M, et al. The effect of the Operating Room Coordinator’s risk appreciation on operating room efficiency. Anesth Analg. 2009;108:1249–56.
Stepaniak PS, Heij C, Mannaerts GH, et al. Modeling procedure and surgical times for current procedural terminology–anesthesia–surgeon combinations and evaluations in terms of case duration prediction and operating room efficiency: a multicenter study. Anesth Analg. 2012;109:1232–45.
Stepaniak PS, Heij C, Mannaerts GH, et al. Bariatric surgery with operating teams that stayed fixed during the day: a multicenter study analyzing the effects on patient outcomes teamwork and safety climate. Anesth Analg. 2012;115:1384–92.
Corn LG, McKenzie M, Pearsal EA, et al. Successful implementation of an enhanced recovery after surgery programme for elective colorectal surgery: a process evaluation of champions’ experience. Implement Sci. 2015;10:99.
Francis NK, Walker T, Carter F, et al. Consensus on training and implementation of enhanced recovery after surgery: a Delphi study. World J Surg. 2018;42:1919–28.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval
Ethical approval for this study was obtained from the scientific board of Tawam Hospital/Johns Hopkins, Al Ain, The United Arab Emirates (AAMDHREC Protocol No. 527-17).
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
G.H.H.M. and R.E.A.A. is combined first author
Rights and permissions
About this article

Cite this article
Mannaerts, G.H.H., Allatif, R.E.A., Al Hashmi, F.Y. et al. First Successful Large-Scale Introduction of an Enhanced Recovery after Bariatric Surgery (ERABS) Program in the Middle East: The Results and Lessons Learned of Tawam Hospital/Johns Hopkins, a Tertiary Governmental Center in the UAE. OBES SURG 29, 2100–2109 (2019). https://doi.org/10.1007/s11695-019-03841-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-03841-4