
Abstract
Summary
Nonagenarians differ from patients aged 70–79 and 80–89 years in baseline characteristics, complication and mortality rates. Differences increased gradually with age. The results of this study can be used, in combination with the Almelo Hip Fracture Score, to deliver efficiently targeted orthogeriatric treatment to the right patient group.
Purpose
In previous literature, elderly with a hip fracture are frequently defined as ≥ 70 years. However, given the ageing population and the rapidly increasing number of ‘nonagenarians’ (aged ≥ 90 years), the question rises whether this definition is still actual. The aim of this study is to determine whether nonagenarians show differences compared to patients aged 70–79 years and patients aged 80–89 years in terms of patient characteristics, complications and mortality rate.
Methods
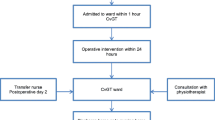
From April 2008 until December 2016, hip fracture patients aged ≥ 70 years treated according to our orthogeriatric treatment model were included. Patients were divided into three different groups based on age at admission: 70–79 years, 80–89 years and ≥ 90 years. Patient characteristics, risk of early mortality, complications and outcomes were analysed. Risk factors for 30-day mortality in nonagenarians were determined.
Results
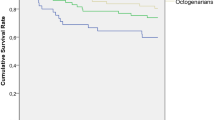
A total of 1587 patients were included: 465 patients aged 70–80 years, 867 patients aged 80–90 years and 255 patients aged ≥ 90 years. Nonagenarians were more often female and had a lower haemoglobin level at admission. Prefracture, they were more often living in a nursing home, were more dependent in activities of daily living and mobility and had a higher risk of early mortality calculated with the Almelo Hip Fracture Score (AHFS). Post-operative, nonagenarians suffer significantly more often from delirium and anaemia. The 30-day mortality and 1-year mortality were significantly higher. Differences increased gradually with age.
Conclusion
Nonagenarians differ from patients aged 70–79 and 80–89 years in baseline characteristics, complication and mortality rates. Differences increased gradually with age. The results of this study can be used, in combination with the Almelo Hip Fracture Score, to deliver efficiently targeted orthogeriatric treatment to the right patient group.


Similar content being viewed by others

References
Hartholt KA, van Beeck EF, Polinder S, van der Velde N, van Lieshout EMM, Panneman MJM, van der Cammen TJM, Patka P (2011) Societal consequences of falls in the older population: injuries, healthcare costs, and long-term reduced quality of life. J Trauma 71:748–753
Cooper C, Campion G, Melton LJ (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2:285–289
Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C (2009) Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int 20:1633–1650
Grigoryan KV, Javedan H, Rudolph JL (2014) Orthogeriatric care models and outcomes in hip fracture patients: a systematic review and meta-analysis. J Orthop Trauma NIH Public Access 28:e49–e55
Folbert EC, Hegeman JH, Vermeer M, Regtuijt EM, van der Velde D, ten Duis HJ, Slaets JP (2017) Improved 1-year mortality in elderly patients with a hip fracture following integrated orthogeriatric treatment. Osteoporos Int 28:269–277
Nijmeijer WS, Folbert EC, Vermeer M, Vollenbroek-Hutten MMR, Hegeman JH (2018) The consistency of care for older patients with a hip fracture: are the results of the integrated orthogeriatric treatment model of the Centre of Geriatric Traumatology consistent 10 years after implementation? Arch Osteoporos 13:131
Zielinski SM, Bouwmans CAM, Heetveld MJ, Bhandari M, Patka P, Van Lieshout EMM (2014) The societal costs of femoral neck fracture patients treated with internal fixation. Osteoporos Int 25:875–885
United Nations, Department of Economic and Social Affairs, Population Division PE and PS. World Population Prospects 2019. Population by Age and Sex (thousands) 2015–2050. https://population.un.org/wpp/DataQuery/. Accessed 12 August 2019
Rivoirard R, Chargari C, Trone J, Falk A, Guy J, Eddekaoui H, Lahmar R, Pacaut C, Mery B, Assouline A, Auberdiac P, Moriceau G, Gonthier R, Guillot A, Merrouche Y, Magné N (2014) General management of nonagenarian patients: a review of the literature. Swiss Med Wkly EMH Media 144:w14059
Ooi LH, Wong TH, Toh CL, Wong HP (2005) Hip fractures in nonagenarians—a study on operative and non-operative management. Injury. 36:142–147
Daruwalla ZJ, Wong KL, Malhotra R, Leong KM, Nee PY, Murphy DP (2016) Hip fracture surgery in nonagenarians-the Devil’s advocate? J Am Geriatr Soc 64:210–211
Dick AG, Davenport D, Bansal M, Burch TS, Edwards MR (2017) Hip fractures in centenarians: has care improved in the National Hip Fracture Database Era? Geriatr Orthop Surg Rehabil 8:161–165
Holt G, Smith R, Duncan K, Hutchison J, Gregori A (2008) Outcome after surgery for the treatment of hip fracture in the extremely elderly. J Bone Jt Surg-Am 90:1899–1905
Jennings AG, de Boer P (1999) Should we operate on nonagenarians with hip fractures? Injury 30:169–172
Shabat S, Mann G, Gepstein R, Fredman B, Folman Y, Nyska M (2004) Operative treatment for hip fractures in patients 100 years of age and older: is it justified? J Orthop Trauma 18:431–435
Tarity TD, Smith EB, Dolan K, Rasouli MR, Maltenfort MG (2013) Mortality in centenarians with hip fractures. Orthopedics. 36:e282–e287
Verma R, Rigby AS, Shaw CJ, Mohsen A (2009) Acute care of hip fractures in centenarians—do we need more resources? Injury 40:368–370
Liu Z, Zhang J, He K, Zhang Y, Zhang Y (2019) Optimized clinical practice for superaged patients with hip fracture: significance of damage control and enhanced recovery program. Burns Trauma 7:21
Prestmo A, Saltvedt I, Helbostad JL, Taraldsen K, Thingstad P, Lydersen S, Sletvold O (2016) Who benefits from orthogeriatric treatment? Results from the Trondheim hip-fracture trial. BMC Geriatr BioMed Central 16:49
Folbert EC, Smit R, van der Velde D, Regtuijt EM, Klaren MH, Hegeman JH (2012) Geriatric fracture center: a multidisciplinary treatment approach for older patients with a hip fracture improved quality of clinical care and short-term treatment outcomes. Geriatr Orthop Surg Rehabil SAGE Publications 3:59–67
Daabiss M (2011) American Society of anaesthesiologists physical status classification. Indian J Anaesth Wolters Kluwer -- Medknow Publ 55:111–115
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Parker MJ, Palmer CR (1993) A new mobility score for predicting mortality after hip fracture. J Bone Joint Surg (Br) 75:797–798
Mahoney FI, Barthel DW (1965) Functional evaluation: the Barthel Index. Md State Med J 14:61–65
Wijnhoven HAH, Schilp J, van Bokhorst-de van der Schueren MAE, de Vet HCW, Kruizenga HM, Deeg DJH, Ferrucci L, Visser M (2012) Development and validation of criteria for determining undernutrition in community-dwelling older men and women: the short nutritional assessment questionnaire 65+. Clin Nutr NIH Public Access 31:351–358
Kristensen MT, Foss NB, Ekdahl C, Kehlet H (2010) Prefracture functional level evaluated by the new mobility score predicts in-hospital outcome after hip fracture surgery. Acta Orthop 81:296–302
Nijmeijer WS, Folbert EC, Vermeer M, Slaets JP, Hegeman JH (2016) Prediction of early mortality following hip fracture surgery in frail elderly: the Almelo Hip Fracture Score (AHFS). Injury. 47:2138–2143
Nordström P, Thorngren K-G, Hommel Phd A, Ziden Phd L, Anttila S (2018) Effects of geriatric team rehabilitation after hip fracture: meta-analysis of randomized controlled trials. J Am Med Dir Assoc 19(10):840–845
Yang Y, Zhao X, Dong T, Yang Z, Zhang Q, Zhang Y (2017) Risk factors for postoperative delirium following hip fracture repair in elderly patients: a systematic review and meta-analysis. Aging Clin Exp Res 29:115–126
Baskaran D, Rahman S, Salmasi Y, Froghi S, Berber O, George M (2018) Effect of tranexamic acid use on blood loss and thromboembolic risk in hip fracture surgery: systematic review and meta-analysis. HIP Int 28:3–10
Hu F, Jiang C, Shen J, Tang P, Wang Y (2012) Preoperative predictors for mortality following hip fracture surgery: a systematic review and meta-analysis. Injury Elsevier Ltd 43:676–685
Maxwell MJ, Moran CG, Moppett IK (2008) Development and validation of a preoperative scoring system to predict 30 day mortality in patients undergoing hip fracture surgery. Br J Anaesth 101:511–517
Belmont PJ, Garcia EJ, Romano D, Bader JO, Nelson KJ, Schoenfeld AJ (2014) Risk factors for complications and in-hospital mortality following hip fractures: a study using the National Trauma Data Bank. Arch Orthop Trauma Surg 134:597–604
Mariconda M, Costa GG, Cerbasi S, Recano P, Aitanti E, Gambacorta M, Misasi M, Mariconda M, Gambacorta M, Misasi M (2015) The determinants of mortality and morbidity during the year following fracture of the hip. Bone Joint J 97-B(3):383–390
Estimated life expectancy at birth, females - European Health Information Gateway. https://gateway.euro.who.int/en/indicators/hfa_72-1092-estimated-life-expectancy-world-health-report-females/. Accessed 23 August 2019
CBS. StatLine - Overledenen; geslacht, leeftijd, burgerlijke staat, regio. https://opendata.cbs.nl/statline/#/CBS/nl/dataset/03747/table?ts=1568381192468. Accessed 23 August 2019
CBS. StatLine - Bevolking; geslacht, leeftijd en burgerlijke staat. https://opendata.cbs.nl/statline/#/CBS/nl/dataset/7461bev/table?ts=1568381326981. Accessed 23 August 2019
Galler M, Zellner M, Roll C, Bäuml C, Füchtmeier B, Müller F (2018) A prospective study with ten years follow-up of two-hundred patients with proximal femoral fracture. Injury. 49:841–845
Pugely AJ, Martin CT, Gao Y, Klocke NF, Callaghan JJ, Marsh JL (2014) A risk calculator for short-term morbidity and mortality after hip fracture surgery. J Orthop Trauma 28:63–69
Cassidy MR, Rosenkranz P, McCabe K, Rosen JE, McAneny D (2013) I COUGH. JAMA Surg Am Med Assoc 148:740
Simunovic N, Devereaux PJ, Sprague S, Guyatt GH, Schemitsch E, DeBeer J, Bhandari M (2010) Effect of early surgery after hip fracture on mortality and complications: systematic review and meta-analysis. Can Med Assoc J 182:1609–1616
Lewis SR, Butler AR, Brammar A, Nicholson A, Smith AF (2016) Perioperative fluid volume optimization following proximal femoral fracture. Cochrane Database Syst Rev 3:CD003004
Polinder S, Haagsma J, Panneman M, Scholten A, Brugmans M, Van Beeck E (2016) The economic burden of injury: health care and productivity costs of injuries in the Netherlands. Accid Anal Prev Pergamon 93:92–100
Lötters FJB, van den Bergh JP, de Vries F, Rutten-van Mölken MPMH (2016) Current and future incidence and costs of osteoporosis-related fractures in the Netherlands: combining claims data with BMD measurements. Calcif Tissue Int 98:235–243
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix. Definitions of complications
Appendix. Definitions of complications
Anaemia: requiring transfusion based on the transfusion guidelines (CBO, 2007)
Arrhythmia: in comparison with electrocardiogram at admission, with need for treatment
Cerebrovascular accident: hemiparesis of hemiplegia, a CT cerebrum is performed
Delirium: based on the Delirium Observation Screening Scale, score above 3 and geriatrician diagnosis confirmed in medical record
Heart failure: clinical presentation and/or diagnosis confirmed on chest radiograph. Treatment started with diuretics
Myocardial infarction: elektrocardiogram abnormalities suspicious for ischemia and elevated cardiac troponin level
Pneumonia: clinical presentation and/or diagnosis confirmed on chest radiograph. Treatment started with antibiotics
Urinary tract infection: urine sediment with positive WBC and nitrite. Treatment started with antibiotics
Wound infection, superficial: diffuse redness, serous fluid leakage and no fever (RIVM, 2014)
Wound infection, deep: worse than superficial, need for revision
Readmission: admission within the first 30 days after discharge
Reoperation: operation within the first 60 days after initial surgery
Implant dislocation: diagnosis confirmed on XR, need for revision
Implant failure: diagnosis confirmed on XR, need for revision
Rights and permissions
About this article

Cite this article
de Groot, R., Nijmeijer, W.S., Folbert, E.C. et al. ‘Nonagenarians’ with a hip fracture: is a different orthogeriatric treatment strategy necessary?. Arch Osteoporos 15, 19 (2020). https://doi.org/10.1007/s11657-020-0698-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-020-0698-7