
Abstract
Summary
Respiratory insufficiency is the leading cause death in people with osteogenesis imperfecta (OI). Adults with OI reported that respiratory symptoms negatively impacted psychosocial wellbeing and limited daily physical activities, irrespective of OI type, age, stature, or scoliosis. The impact of respiratory status on quality of life in this population warrants further investigation.
Purpose
Respiratory insufficiency is the leading cause of mortality in osteogenesis imperfecta (OI), a heterogeneous group of heritable connective tissue disorders characterized by fractures, bone fragility, and scoliosis. There is little research on how respiratory health influences daily life in this population. This study explores the relationship between respiratory function and quality of life in adults with OI.
Methods
One hundred fifty-seven adults with OI completed the St. George’s Respiratory Questionnaire (SGRQ) and provided demographic and health information through REDCap. SGRQ scores were compared to reference scores for the general population, and comparisons were made between OI type, presence of scoliosis, stature, and other factors such as age or comorbidities.
Results
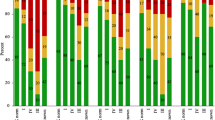
Average age was 45.87 years (range 19–81). Respondents scored worse on average (32 ± 23) than the normative data (6 ± 1). Those with type I OI scored better than those with type IV (p = 0.002) or type III (p = 0.024). Total scores correlated with age, activity level, assistive device use, and presence of pulmonary or cardiac comorbidities but did not correlate with stature or degree of scoliosis.
Conclusion
Respiratory symptoms negatively impact both psychosocial wellbeing in the OI population and limit daily physical activity. These limitations occur irrespective of their OI type, age, stature, or scoliosis and reflect the dramatic impact of respiratory status on quality of life for people with OI. Future studies should examine the etiology of respiratory insufficiency in this population so guidelines for management can be established.
Similar content being viewed by others


References
Tauer JT, Robinson ME, Rauch F (2019) Osteogenesis imperfecta: new perspectives from clinical and translational research. JBMR Plus e10174
Sykes B, Ogilvie D, Wordsworth P (1986) Anderson, Jones N, Osteogenesis imperfecta is linked to both type I collagen structural genes. Lancet. 2:69–72
Patel RM, Nagamani SC, Cuthbertson D, Campeau PM, Krischer JP, Shapiro JR, Steiner RD, Smith PA, Bober MB, Byers PH, Pepin M, Durigova M, Glorieux FH, Rauch F, Lee BH, Hart T, Sutton VR (2015) A cross-sectional multicenter study of osteogenesis imperfecta in North America - results from the linked clinical research centers. Clin Genet. 87:133–140
Sillence D, Senn A, Danks DM (1979) Genetic heterogeneity in osteogenesis imperfecta. J Med Genet 16(2):101–116
Van Dijk FS, Sillence DO (2014) Osteogenesis imperfecta: clinical diagnosis, nomenclature and severity assessment. American journal of medical genetics Part A. 164(6):1470–1481
Sillence DO, Rimoin DL, Danks DM (1979) Clinical variability in osteogenesis imperfecta variable expressivity or genetic heterogeneity. Birth Defects Orig Artic Ser 15:113–129
Gajko-Galicka A (2002) Mutations in type I collagen genes resulting in osteogenesis imperfecta in humans. Acta Biochimica Polonica. 49(2):433–441
Hald JD, Folkestad L, Swan CZ, Wanscher J, Schmidt M, Gjørup H, Haubek D, Leonhard CH, Larsen DA, Hjortdal JØ, Harsløf T, Duno M, Lund AM, Jensen JB, Brixen K, Langdahl B (2018) Osteogenesis imperfecta and the teeth, eyes, and ears—a study of non-skeletal phenotypes in adults. Osteoporosis International. 29(12):2781–2789
Laurent GJ (1986) Lung collagen: more than scaffolding. Thorax. 41(6):418–428
McAllion SJ, Paterson CR (1996) Causes of death in osteogenesis imperfecta. J Clin Pathol 49:627–630
Rauch F, Glorieux FH (2004) Osteogenesis imperfecta. Lancet (London, England) 363:1377–1385
Sandhaus RA (2014) Chapter 35-Pulmonary function in osteogenesis imperfecta. Shapiro JR, Byers PH, Glorieux FH, Sponseller PD (eds). Osteogenesis imperfecta: a translational approach to brittle bone disease. pp 335–342
Thibeault DW, Pettett G, Mabry SM, Rezaiekhaligh MM (1995) Osteogenesis imperfecta type IIA and pulmonary hypoplasia with normal alveolar development. Pediatr Pulmonol 20:301–306
Falvo KA, Root L, Bullough PG (1974) Osteogenesis imperfecta: clinical evaluation and management. J Bone Joint Surg Am 56:783–793
Norimatsu H, Mayuzumi T, Takahashi H (1982) The development of the spinal deformities in osteogenesis imperfecta. Clin Orthop Relat Res. 165:20–25
Wekre LL, Kjensli A, Aasand K, Falch JA, Eriksen EF (2014) Spinal deformities and lung function in adults with osteogenesis imperfecta. Clin Respir J 8:437–443
Bronheim R, Khan S, Carter E, Sandhaus RA, Raggio C (2019) Scoliosis and cardiopulmonary outcomes in osteogenesis imperfecta patients. Spine 44:1057–1063
Widmann RF, Bitan FD, Laplaza FJ, Burke SW, DiMaio MF, Schneider R (1999) Spinal deformity, pulmonary compromise, and quality of life in osteogenesis imperfecta. Spine 24:1673–1678
Himakhun W, Rojnueangnit K, Prachukthum S (2012) Perinatal lethal osteogenesis imperfecta in a Thai newborn: the autopsy and histopathogical findings. J Med Assoc Thail. 95:190–194
Shapiro JR, Burn VE, Chipman SD, Jacobs JB, Schloo B, Reid L, Larsen N, Louis F (1989) Pulmonary hypoplasia and osteogenesis imperfecta type II with defective synthesis of alpha I(1) procollagen. Bone. 10:165–171
Ferrer M, Villasante C, Alonso J, Sobradillo V, Gabriel R, Vilagut G, Masa JF, Viejo JL, Jiménez-Ruiz CA, Miravitlles M (2002) Interpretation of quality of life scores from the St. George’s Respiratory Questionnaire. Eur Respir J 19:405–413
Jones PW, Forde Y (2009) St George’s Respiratory Questionnaire Manual. University of London, London
Yonko E, Carter E, Sandhaus R, Raggio C (2019) Respiratory health impacts quality of life for adults with OI [abstract]. Presented at the 9th International Conference on Children’s Bone Health, Salzburg, Austria. Bone Abstracts. 7:P105
Osteogenesis Imperfecta Foundation (n.d.) Current studies. Retrieved from https://oif.org/currentstudies/. Accessed 15 June 2020
Survey on Respiratory Function & OI (2019) OIFE Magazine, p. 25
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG (2009) Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42:377–381
Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, McLeod L, Delacqua G, Delacqua F, Kirby J, Duda SN, REDCap Consortium (2019) The REDCap consortium: building an international community of software partners. J Biomed Inform 95:103208
Jones PW (2002) Interpreting thresholds for a clinically significant change in health status in asthma and COPD. European Respiratory Journal. 19:398–404
Swezey T, Reeve BB, Hart TS, Floor MK, Dollar CM, Gillies AP, Tosi LL (2019) Incorporating the patient perspective in the study of rare bone disease: insights from the osteogenesis imperfecta community. Osteoporos Int. 30(2):507–511. https://doi.org/10.1007/s00198-018-4690-7
Acknowledgments
The researchers would like to thank the Osteogenesis Imperfecta Foundation (OIF), Brittle Bone Disorder Consortium, and Osteogenesis Imperfecta Federation Europe (OIFE) for circulating recruitment materials for this study. The researchers would also like to thank Kathryn O. and Alan C. Greenberg for their ongoing support of the Center for Skeletal Dysplasias at Hospital for Special Surgery. Finally, we would like to acknowledge members of the OI community who participated in this study.
Availability of data and material
Due to the nature of this research study, investigators did not obtain permission from study participants for their data to be shared publicly. Therefore, no supporting data is available.
Funding
Financial support for dissemination of research reported in this publication was received from the Osteogenesis Imperfecta Foundation Jamie Kendall Fund for Adult OI Health. Research reported in this publication was supported by the National Center For Advancing Translational Science of the National Institute of Health Under Award Number UL1TR002384. This study was also supported by the Osteogenesis Imperfecta Foundation. This study utilized the Brittle Bone Disorders Consortium Contact Registry, hosted by the Rare Diseases Clinical Research Network. The Brittle Bone Disease Consortium (1U54AR068069-0) is a part of the National Center for Advancing Translational Sciences (NCATS) Rare Diseases Clinical Research Network (RDCRN) and is funded through a collaboration between the Office of Rare Diseases Research (ORDR), NCATS, the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), the National Institute of Dental and Craniofacial Research (NIDCR), and the Eunice Kennedy Shriver National Institutes of Child Health and Development (NICHD). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
All authors provide substantial contributions to research design, or the acquisition, analysis, or interpretation of data. All authors drafted the paper or revise it critically. All authors approved the submitted and final versions. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflicts of interest
Cathleen L. Raggio received support from the Osteogenesis Imperfecta Foundation to cover dissemination fees associated with this research. Elizabeth A. Yonko, Jillian S. Emanuel, Erin M. Carter, and Robert A. Sandhaus declare that they have no conflict of interest.
Ethics approval
All work was performed at Hospital for Special Surgery, NY, NY and National Jewish Health in Denver, CO. This study was performed in accordance with the ethical standards in the 1964 Declaration of Helsinki and regulations of HIPAA. Details that might disclose the identity of the subjects under study were omitted. IRB approval was obtained at Hospital for Special Surgery.
Consent to participate
The requirement for consent to participate was waived by Hospital for Special Surgery’s Institutional Review Board because the research involved no more than minimal risk to subjects, did not adversely affect rights and welfare of subjects, and could not practicably be carried out without the waiver.
Consent for publication
Consent for publication was not obtained for the same reasons as listed above. The publication does not contain any identifying information.
Code availability
Not applicable
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yonko, E.A., Emanuel, J.S., Carter, E.M. et al. Respiratory impairment impacts QOL in osteogenesis imperfecta independent of skeletal abnormalities. Arch Osteoporos 15, 153 (2020). https://doi.org/10.1007/s11657-020-00818-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-020-00818-0