
Abstract
We present our experience over the long-term of monitoring of visual function in children with craniopharyngioma. Our study involves an analysis of all paediatric patients with craniopharyngioma younger than 16 at the time of diagnosis and represents a series of predominantly sub-totally resected tumours. Visual data, of multiple modality, of the paediatric patients was collected. Twenty patients were surveyed. Poor prognostic indicators of the visual outcome and rate of recurrence were assessed. Severe visual loss and papilledema at the time of diagnosis were more common in children under the age of 6. In our study visual signs, tumour calcification and optic disc atrophy at presentation are predictors of poor visual outcome with the first two applying only in children younger than 6. In contrast with previous reports, preoperative visual field (VF) defects and type of surgery were not documented as prognostic indicators of poor postoperative visual acuity (VA) and VF. Contrary to previous reports calcification at diagnosis, type of surgery and preoperative VF defects were not found to be associated with tumour recurrence. Local recurrence is common. Younger age at presentation is associated with a tendency to recur. Magnetic resonance imaging (MRI) remains the recommended means of follow-up in patients with craniopharyngioma.
Similar content being viewed by others

Introduction
Craniopharyngiomas are benign epithelial tumours arising from remnants of the Rathke’s pouch. They account only for 2–5 % of all intracranial neoplasms [1] and are usually located in the sellar and suprasellar region. Their proximity to the optic pathways and vital structures of the brain may give rise to a variety of visual signs and systemic symptoms resulting from raised intracranial pressure and disruption of the hypothalamic pituitary axis [2, 3].
Despite their benign histological appearance with survival rates in the order of 91–98 % [4], their prognosis and long-term outcome may be poor and unfavorable as a consequence of the tumour’s location and subsequent treatment [5]. 70 % of patients have visual signs at presentation whereas children tend to present with systemic symptoms with headache being the most commonly recorded complaint [6].
The debate regarding the optimal management of craniopharyngiomas is ongoing and controversial in relation to the benefit of complete removal compared to less aggressive surgery combined with radiotherapy [7, 8].
Several reports have assessed visual acuity (VA) and visual field (VF) preoperatively and in the early postoperative period [9–12]. Although immediate postoperative VA correlates with the severity of reduced preoperative VA, few reports have examined progression over time [10, 11].
The aim of this study is to present our experience over the long-term of monitoring of visual function in children with craniopharyngioma. Tumors` natural history with regard to their effects on the visual system was investigated in patients younger than 16 at presentation. In addition to this poor prognostic indicators of the postoperative visual outcome and recurrence were assessed. This study represents a series of predominantly sub-totally resected tumors.
Materials and methods
A search in the paediatric oncology database at our institution, St James University Hospital, was performed allowing identification of all paediatric patients with craniopharyngioma attending the joint paediatric ophthalmology-neurooncology clinic.
Data was collected from the pre-surgical and post-surgical ophthalmic examination and at last follow-up. These included best corrected visual acuity (BCVA) in all children using either Logmar or Preferential Looking charts based on patient’s age. Both methods are quantitative and facilitate better descriptions of VA changes [13]. VF was tested with Goldmann perimetry. Visual data of half of the paediatric patients was prospectively collected over an 8-year period between 2004 and 2012 whereas data of the rest of the cohort was collected retrospectively.
The data was converted to an 8-point scale with 8 representing good visual function and 1 representing poor visual function (Table 1). VA was classified as normal if BCVA was equal to grade 8 as defined by the 8-point scale. Severe visual loss was documented if BCVA was equal or worse to grade 4 according to the provided scale. Difference by one grade was the minimum amount of change required for the visual outcomes to be classified as improved or worse.
Two age groups were generated with boundary being the age of 6. Visual data of multiple modality were compared in order to identify differences between outcomes of young versus older children. Sex, age, presenting symptoms, duration of symptoms, surgical procedures and number of recurrences were also reviewed.
Contingency tables data were analyzed using Fisher’s exact test while the comparison between the means was performed using the t test. Clinical significance was accepted for P values less than 0.05.
Results
Patient characteristics
Twenty patients (10 male and 10 female) were included with a mean age at diagnosis of 7.3 years (range 1.25–13.75 years). 10 patients were aged less than 6 years (6 male, 4 female) with a median age of 4.1 years and 10 patients were aged older than 6 (4 male, 6 female) with a median age 10.6 years. The mean follow-up period since presentation in this cohort was 156.95 months with a range from 26 months to 413 months.
Symptoms
Headache was the most frequent systemic complaint occurring in 14 patients (70 %). Visual symptoms were present at diagnosis in 12 children (60 %). Loss of VA was the most common ocular complaint present in 6 patients (30 %). VA deficits at the time of diagnosis were found in 52.5 % of children similar to the finding of the 51.7 % of patients by Defoort-Dhellemmes et al. [14].
The duration of symptoms prior to admission ranged from 10 days to 3 years with a mean duration of 2 weeks for visual symptoms, whereas systemic symptoms had a mean duration of 6 months (range 1 month to 3 years). The ratio of patients with systemic symptoms to visual symptoms was not significant between the 2 age groups.
Visual acuity
Table 2 presents VA at initial presentation and at last follow-up divided into three groups showing the number of eyes in each group. Severe visual loss at presentation was more frequently recorded in children younger than 6 (P = 0.0004, Fisher’s exact test). In contrast children aged >6 years tend to present with normal VA in a significant higher rate (P = 0.0104, Fisher’s exact test). At final review VA improved in 8 eyes (20 %), remained stable in 24 eyes (60 %) and deteriorated in 8 eyes (20 %).
Visual signs at the time of diagnosis were present in 12 patients (6 children aged <6 and 6 children aged >6). Among patients presented with visual signs poor postoperative VA was more frequently documented in children aged <6 (P = 0.0391, Fisher’s exact test).
Visual field
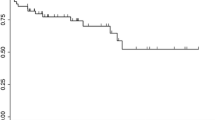
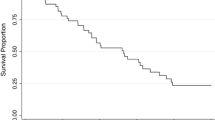
Fourteen out of the 20 patients (4 aged <6 and 10 aged >6) were able to perform Goldmann perimetry testing. At initial presentation bitemporal hemianopia was the most common VF defect occurring in 5 patients (35.7 %) with no difference between the 2 age groups (P = 0.87, t-test). This is not surprising given craniopharyngioma’s location and growth in relation to the chiasm. VF were normal in 4 patients (28.5 %), all were older than 6 years of age. Analysis of the VF at initial presentation and at final review showed that 5 improved (35.7 %), 5 remained unchanged (35.7 %) and 4 showed deterioration (28.5 %). Pleomorphism described as the change from one type of field defect to another was demonstrated in 3 patients (15 %). Figure 1 shows VF at presentation and at final review of all 20 patients included in the study.

VF of the cohort at initial presentation and at last follow-up converted to the 8-point scale
64.7 % of the eyes presenting with VF defects had normal VA at final review (P = 0.0549, Fisher’s exact test). 41.1 % of the eyes with initial VF defects demonstrated VF improvement in the long-term (P = 0.01806, t test).
Fundoscopy
Optic atrophy was present at the time of diagnosis in 12 patients (60 %). Six patients (30 %) had bilateral papilledema. Optic disc atrophy at presentation was associated with poor visual outcome (P = 0.0662, Fisher’s exact test). Better preoperative VA was recorded in children with papilledema at the time of diagnosis (P = 0.0248, Fisher’s exact test). At last review optic disc pallor was documented in 18 patients (90 %).
Tumour characteristics
All the tumours were suprasellar in location. Ten were cystic masses and 10 had both cystic and solid components. There was no difference in tumour consistency between the 2 age groups. (P = 0.6563, Fisher’s exact test) Tumor consistency and location were not found to impact on the visual outcome. No significant difference was recorded in postoperative VA among tumors with prechiasmatic and retrochiasmatic extension.
Calcified components of the tumour on diagnostic neuroimaging were detected in 60 % of the children with no difference in the rate between the 2 age groups. In our study we found that calcification at presentation may be associated with poor postoperative VA only in children under the age of 6 (P = 0.0472, Fisher’s exact test).
Management
All patients but one received surgical removal of the tumour. Initial surgery, surgical approach and rate of recurrence in both age groups are shown in Table 3. At our institution gross total resection was performed in only 7 patients, while 12 patients underwent subtotal resection of the tumor with no difference between the 2 age groups. Transcranial surgery was performed in all patients whereas none received transsphenoidal surgery. Pterional approach was preferred in 12 patients (63.1 %) while the remainder undergone initial surgery through sub-frontal approach. Postoperatively no difference was recorded in the visual outcomes between children treated with either total or partial resection (P = 0.7396, Fisher’s exact test).
Nine patients underwent radiotherapy as part of their initial management due to incomplete tumour resection. Most children received radiation therapy were older than 6 avoiding the significant risks of irradiation in the younger group. The impact of radiotherapy on the visual outcome was not found to be significant (P = 0.7547, Fisher’s exact test). Mean duration between initial surgery and subsequent radiotherapy was 4.4 months (range 2–7 months). No serious adverse effects occurred during the course of irradiation.
Tumour recurrence
Eleven patients (55 %) experienced recurrence of whom only 2 had more than one episode. Age less than 6 years was associated with recurrence (n = 8, P = 0.0698, Fisher’s exact test). Mean duration between surgery and first recurrence was 13 months (range 4–48 months). All patients underwent repeat surgical approach while 5 required further radiotherapy.
Headache was the most common presentation at the time of recurrence occuring in 5 patients (45.5 %). Recurrence of tumour was picked up in 3 children who presented with deterioration of VA and VF (27.2 %). Three patients had asymptomatic radiological progression which was identified on surveillance MRI scan.
No difference was recorded in the rate of recurrence between children treated with either total or partial resection (P = 0.3765, Fisher’s exact test) in contrast with previous study where complete resection is associated with excellent tumour control [15]. Total number of recurrence was not found to impact on poor visual outcome. Nineteen of the 20 patients are still under regular ophthalmological review whereas one patient is deceased.
Discussion
Craniopharyngioma’s size, location and extension accounts for it’s varying presentation. In our study poor preoperative VA was associated only with age younger than 6 years similar to previous reports [6, 10]. Postoperatively the number of children presenting with poor VA remained unchanged in both age groups. This observation confirms that age less than 6 is an unfavorable predictor of the visual outcome as addressed by Abrams et al. [12], but not attributable to progressive visual loss during the long-term follow-up as many of the children of this age group already experience poor vision by the time of diagnosis. This may be due to late presentation which leads in delay in diagnosis and higher visual morbidity.
In our study visual signs at presentation were associated with poor visual outcome only in children younger than 6. In contrast previous studies commented that visual signs at the time of diagnosis were predictors of poor postoperative VA in all children less than 18 years of age [12].
Contrary to previous report preoperative VF defects were not found to be prognostic indicators of poor postoperative VA and VF [16] as most eyes with initial VF defects tend to preserve better VA and VF postoperatively. However the evaluation of the data in the previous study was based on the number of patients in contrast to the number of eyes.
At presentation optic atrophy was more common than disc swelling and was found to be an important prognostic factor of poor visual outcome in patients with craniopharyngioma. Papilledema was more common in children under the age of 6 whereas Repka et al. [10] suggested that was more frequent in children than adults.
Calcification at presentation was found to be poor prognostic indicator of the visual outcome in children younger than 6. Therefore lack of calcification on neuroimaging at the time of diagnosis may be encouraging for the visual prognosis in children of this age group.
The optimal therapeutic approach of craniopharyngiomas continues to polarize options amongst surgeons with some suggesting complete removal of the tumour only if hypothalamic morbidity is acceptably low [17], whereas others advocate limited surgery supplemented by radiotherapy. Both treatment strategies yield similar rates of overall survival [18, 19]. However, irradiation is often associated with detrimental effects, including hypothalamic-pituitary axis dysfunction, cognitive morbidity, radiation induced CNS tumours and progressive decline of IQ [20, 21]. These effects were found to be more pronounced in patients under 5 years of age [22]. Given the increased morbidity and inability to depend on radiotherapy in this vulnerable population several authors agree with radical resection by an experienced surgeon as the optimal management of very young children with craniopharyngioma [23–25].
However, at our institution gross total resection confirmed by intraoperative inspection and postoperative imaging was not the mainstream treatment approach. Most children underwent subtotal resection of the tumour mainly due to vascular involvement and significant calcification densely adherent to posterior communicating arteries and carotid. This is likely responsible for the increased recurrence rate found in our study compared to most series. Given the increased risk of radiotherapy side effects in the very young population, adjuvant radiation therapy was mainly offered in children older than 6 years of age.
Surgical treatment with craniotomy is especially useful for craniopharyngiomas with suprasellar and parasellar extension [26]. In our study none of the patients received endoscopic transsphenoidal surgery as all craniopharyngiomas had an extrasellar component and transcranial surgery was performed in all the cases. Most children undergone initial surgery through the extended pterional approach.
In our study no difference was recorded in the visual outcomes between children treated with either total or partial resection, while the impact of surgery and radiotherapy on the visual outcome was not found to be significant. Previous reports demonstrated less postoperative visual acuity deficits following transcranial surgery compared to the transsphenoidal group [27], whereas others advocated better visual outcomes with the endoscopic endonasal approach [28]. However, in our study comparable results are not available as no one received skull base approach. Preoperative presence of hydrocephalus, 3rd ventricular invasion as well as total number of operations including ventriculo-peritoneal shunting were not found to be predictors of the final VA.
In our study younger age at presentation was associated with a tendency to recur. Variables such as radiotherapy, preoperative presence of hydrocephalus and 3rd ventricular invasion were not found to impact on recurrence rate. In contrast with previous report no difference was recorded in the rate of recurrence between children treated with either total or partial resection [15]. Elliott et al. [23] demonstrated decreased recurrence rate in children aged less than 6 years following radical resection of tumour. We did not find similar association. However, the number of children underwent gross total resection in our study was significantly low.
Fisher et al. [11] advocates that lack of calcification at diagnosis is associated with a tendency to remain free of relapse. In contrast in our study no difference was found in the recurrence rate between children with or without calcified components of the tumour at the time of diagnosis. Previous reports commented that residual calcification does not have an impact on the risk of recurrence after radical resection in paediatric craniopharyngiomas [29]. All poor prognostic indicators of the visual outcome and recurrence are outlined in Table 4.
MRI remains the recommended means of follow-up in a patient with craniopharyngioma. The UK consensus guidelines recommend MRI surveillance at 6-month intervals [30] whereas most centers in North America suggest neuroimaging within 2 years after definitive treatment as most tumours tend to recur beyond this period. VA and VF testing are useful tools in monitoring for recurrence. However, their role in diagnosis should not be overestimated and cannot replace radiographic imaging since by the time that tumour causes new visual deterioration, it is sizable and the likelihood of retrieval therapy is significantly diminished.
Limitations of this study include the relative small number of children that were surveyed that may prevent us from reaching firm conclusions while the cohort of the population was collected from a single care center in contrast with multicenter studies. The extreme young age in a few cases precluded reliable vision examinations as subjects younger than 3 years old are inevitably difficult to examine resulting in some incomplete data on some of the visual outcomes. VA is a psychological measure, since it relies heavily on the patient’s cooperation and attention. Moreover accuracy of the results can be compromised by comorbid attention deficit-hyperactivity disorder commonly seen in children with craniopharyngioma.
However, a standardised VA assessement was employed in our center providing consistency from study enrollment through study completion. Since in younger children, scoring one line better or worse on repeat testing is not uncommon, a two-line or one-grade decline in VA according to Table 1 was recommended as sufficient to describe change. VF testing was difficult to perform in children aged <6. However, previous reports have documented the reliability of VF examination in children as young as the age of 4 [31, 32].
In summary, our study assessed the natural history and the visual outcomes of 20 children with craniopharyngioma over a long-term period. Poor prognostic indicators of the visual outcome and rate of recurrence were assessed. Optic disc atrophy at presentation was found to be associated with poor visual outcome while visual signs and tumour calcification at the time of diagnosis were documented as poor predictors only in children younger than 6. In contrast with previous reports, preoperative VF defects and type of surgery were not associated with poor postoperative VA and VF. Contrary to previous reports calcification at diagnosis, type of surgery and preoperative VF defects were not found to be associated with tumour recurrence. Although VA and VF are useful tools in monitoring for recurrence MRI remains the recommended means of follow-up.
References
Parisi JE, Mena H (1993) Non glial tumours. In: Nelson JS, Parisi JE, Schochet SSJ (eds) Principles and practice of neuropathology. Mosby, St Louis, pp 203–266
Van Effenterre R, Boch AL (2002) Craniopharyngioma in adults and children: a study of 122 surgical cases. J Neurosurg 97:3–11
Honegger J, Buchfelder M, Fahlbusch R (1990) Surgical treatment of craniopharyngiomas: endocrinological results. J Neurosurg 90:251–257
Müller HL (2011) Consequences of craniopharyngioma surgery in children. J Clin Endocrinol Metab 96:1981–1991
Pereira AM, Schmid EM, Schutte PJ et al (2005) High prevalence of long-term cardiovascular, neurological and psychosocial morbidity after treatment for craniopharyngioma. Clin Endocrinol Oxf 62:197–204
Chen C, Okera S, Davies PE et al (2003) Craniopharyngioma: a review of long-term visual outcome. Clin Exp Ophthalmol 31:220–228
Vinchon M, Weill J, Delestret I et al (2009) Craniopharyngioma and hypothalamic obesity in children. Childs Nerv Syst 25:347–352
Pierre-Kahn A, Recassens C, Pinto G et al (2005) Social and psycho-intellectual outcome following radical removal of craniopharyngiomas in childhood. A prospect series. Childs Nerv Syst 21:817–824
Khafaga Y, Jenkin D, Kanaan I et al (1998) Craniopharyngioma in children. Int J Radiat Oncol Biol Phys 42:601–606
Repka MX, Miller NR, Miller M (1989) Visual outcome after surgical removal of craniopharyngiomas. Ophthalmology 96:195–199
Fisher PG, Jenab J, Gopldthwaite PT et al (1998) Outcomes and failure patterns in childhood craniopharyngiomas. Childs Nerv Syst 14:558–563
Abrams LS, Repka MX (1997) Visual outcome of craniopharyngioma in children. J Pediatr Ophthalmol Strabismus 34:223–228
Avery RA, Ferner RE, Listernick R et al (2012) Visual acuity in children with low grade gliomas of the visual pathway: implications for patient care and clinical research. J Neurooncol 110:1–7
Defoort-Dhellemmes S, Moritz F, Bouacha I et al (2006) Craniopharyngioma: ophthalmological aspects at diagnosis. J Pediatr Endocrinol Metab 19:321–324
Karavitaki N, Brufani C, Warner JT et al (2005) Craniopharyngiomas in children and adults: systematic analysis of 121 cases with long-term follow-up. Clin Endocrinol Oxf 62:397–409
Lee MJ, Hwang JM (2012) Initial visual field as a predictor of recurrence and postoperative visual outcome in children with craniopharyngioma. J Pediatr Ophthalmol Strabismus 49:38–42
Albright AL, Hadjipanayis CG, Lunsford LD et al (2005) Individualized treatment of pediatric craniopharyngiomas. Childs Nerv Syst 21:649–654
Kalapurakal JA, Goldman S, Hsieh YC et al (2003) Clinical outcome in children with craniopharyngioma treated with primary surgery and radiotherapy deferred until relapse. Med Pediatr Oncol 40:214–218
Puget S, Garnett M, Wray A et al (2007) Pediatric craniopharyngiomas: classification and treatment according to the degree of hypothalamic involvement. J Neurosurg 106:3–12
Anderson VA, Godber T, Smibert E et al (2004) Impairments of attention following treatment with cranial irradiation and chemotherapy in children. J Clin Exp Neuropsychol 26:684–697
Spiegler BJ, Bouffet E, Greenberg ML et al (2004) Change in neurocognitive functioning after treatment with cranial radiation in childhood. J Clin Oncol 22:706–713
Neglia JP, Robison LL, Stovall M et al (2006) New primary neoplasms of the central nervous system in survivors of childhood cancer: a report from the childhood cancer survivor study. J Natl Cancer Inst 98:1528–1537
Elliott RE, Wisoff JH (2009) Successful surgical treatment of craniopharyngioma in very young children. J Neurosurg Pediatr 3:397–406
Vinchon M, Dhellemmes P (2008) Craniopharyngiomas in children: recurrence, reoperation and outcome. Childs Nerv Syst 24:211–217
Thompson D, Phipps K, Hayward R (2005) Craniopharyngioma in childhood: our evidence-based approach to management. Childs Nerv Syst 2:660–668
Tamasauskas A, Bunevicius A, Matukevicius A et al (2014) Extended pterional approach for initial surgical management of craniopharyngiomas: a case series. Turk Neurosurg 24:174–183
Elliott RE, Jane JA Jr, Wisoff JH (2011) Surgical management of craniopharyngiomas in children: meta-analysis and comparison of transcranial and transsphenoidal approaches. Neurosurgery 69:630–643
Komotar RJ, Starke RM, Raper DM et al (2012) Endoscopic endonasal compared with microscopic transsphenoidal and open transcranial resection of craniopharyngiomas. World Neurosurg 77:329–341
Elliott RE, Moshel YA, Wisoff JH (2009) Minimal residual calcification and recurrence after gross-total resection of craniopharyngioma in children. J Neurosurg Pediatr 3:276–283
Spoudeas HA (2005) Paediatric endocrine tumours. A multi-disciplinary consensus statement of best practice from a working group convened under the auspices of the BSPED and UKCCSG. Novo Nordisk Ltd, Crawley
Quinn GE, Fea AM, Minguini N (1991) Visual fields in 4- to 10-year-old children using Goldmann and double-arc perimeters. J Pediatr Ophthalmol Strabismus 28:314–319
Safran AB, Laffi GL, Bullinger A et al (1996) Feasibility of automated visual field examination in children between 5 and 8 years of age. Br J Ophthalmol 80:515–518
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
The study complies with the current laws of the country.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Drimtzias, E., Falzon, K., Picton, S. et al. The ophthalmic natural history of paediatric craniopharyngioma: a long-term review. J Neurooncol 120, 651–656 (2014). https://doi.org/10.1007/s11060-014-1600-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-014-1600-5