
Summary
Background
The intention of the first ileocolic resection in Crohn’s disease is to remove local disease, which relieves symptoms of intestinal obstruction, but should also relieve clinically significant systemic inflammation and allow discontinuation of corticosteroids.
Methods
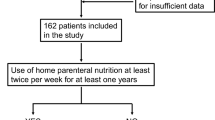
By means of five clinically relevant criteria for continued specific treatment, we evaluated the response of 117 patients to their first ileocolic resection for Crohn’s disease, which was undertaken at Karolinska University Hospital, Stockholm, Sweden, between 2000 and 2010. The five criteria were the persistence of systemic inflammation and continued or resumed corticosteroid therapy, high defecation frequency or presence of a stoma, and the need for new bowel surgery within 1 year. The presence of systemic inflammation and use of anti-inflammatory drugs were assessed 1 month preoperatively and 6–12 months after surgery. Other events of interest were assessed within 12 months.
Results
The median age was 31 years and 51 patients (44 %) were women. In all, 54 patients (46 %) were operated on within the first year of diagnosis and episodes of bowel obstruction were the prime surgical indication in 80 (68 %) patients. Of the patients, 100 (85 %) had an ileocolic resection and 17 (15 %) had terminal ileal surgery. As anticipated, C‑reactive protein (CRP), albumin, and hemoglobin concentrations all normalized significantly after surgery but 15 (13 %) patients still had CRP values of ≥ 30 mg/l and one fourth (29/117, 25 %) still used corticosteroids. Seventeen patients (15 %) had six or more defecations per day or a temporary stoma and four (3 %) patients had new surgery for symptomatic Crohn’s disease. Altogether, 46 (39 %) patients met one or more of the criteria for continued or renewed treatment within 1 year with a higher risk in patients with ileocolic disease as compared with ileal disease when adjusted for age and reoperation (p = 0.030).
Conclusion
The curable intention of the first ileocolic resection for Crohn’s disease often fails, as the need for continued or renewed medical or surgical treatment in the first year is high.
Similar content being viewed by others

References
Lapidus A, Bernell O, Hellers G, Persson PG, Lofberg R. Incidence of crohn’s disease in stockholm county 1955–1989. Gut. 1997;41:480–6.
Sjoberg D, Holmstrom T, Larsson M, Nielsen AL, Holmquist L, Ekbom A, Ronnblom A. Incidence and clinical course of crohn’s disease during the first year – results from the ibd cohort of the uppsala region (icure) of sweden 2005–2009. J Crohns Colitis. 2014;8:215–22.
Bernell O, Lapidus A, Hellers G. Risk factors for surgery and recurrence in 907 patients with primary ileocaecal crohn’s disease. Br J Surg. 2000;87:1697–701.
Henriksen M, Jahnsen J, Lygren I, Stray N, Sauar J, Vatn MH, Moum B, Group IS. C‑reactive protein: A predictive factor and marker of inflammation in inflammatory bowel disease. Results from a prospective population-based study. Gut. 2008;57:1518–23.
Reimund JM, Arondel Y, Escalin G, Finck G, Baumann R, Duclos B. Immune activation and nutritional status in adult crohn’s disease patients. Dig Liver Dis. 2005;37:424–31.
Bager P, Befrits R, Wikman O, Lindgren S, Moum B, Hjortswang H, Dahlerup JF. The prevalence of anemia and iron deficiency in ibd outpatients in scandinavia. Scand J Gastroenterol. 2011;46:304–9.
Burisch J, Pedersen N, Cukovic-Cavka S, Turk N, Kaimakliotis I, Duricova D, Shonova O, Vind I, Avnstrom S, Thorsgaard N, Krabbe S, Andersen V, Dahlerup JF, Kjeldsen J, Salupere R, Olsen J, Nielsen KR, Manninen P, Collin P, Katsanos KH, Tsianos EV, Ladefoged K, Lakatos L, Bailey Y, O’Morain C, Schwartz D, Odes S, Martinato M, Lombardini S, Jonaitis L, Kupcinskas L, Turcan S, Barros L, Magro F, Lazar D, Goldis A, Nikulina I, Belousova E, Fernandez A, Hernandez V, Almer S, Zhulina Y, Halfvarson J, Tsai HH, Sebastian S, Lakatos PL, Langholz E, Munkholm P, EpiCom G. Initial disease course and treatment in an inflammatory bowel disease inception cohort in europe: The ecco-epicom cohort. Inflamm Bowel Dis. 2014;20:36–46.
D’Haens G, Baert F, Assche G van, Caenepeel P, Vergauwe P, Tuynman H, De Vos M, Deventer S van, Stitt L, Donner A, Vermeire S, Van de Mierop FJ, Coche JC, Woude J van der, Ochsenkuhn T, Bodegraven AA van, Van Hootegem PP, Lambrecht GL, Mana F, Rutgeerts P, Feagan BG, Hommes D, Belgian Inflammatory Bowel Disease Research G, North-Holland Gut C. Early combined immunosuppression or conventional management in patients with newly diagnosed crohn’s disease: An open randomised trial. Lancet. 2008;371:660–7.
Sakatani A, Fujiya M, Ito T, Inaba Y, Ueno N, Kashima S, Tominaga M, Moriichi K, Okamoto K, Tanabe H, Ikuta K, Ohtake T, Kono T, Furukawa H, Ashida T, Kohgo Y. Infliximab extends the duration until the first surgery in patients with crohn’s disease. Biomed Res Int. 2013;2013:879491.
Regueiro M, Schraut W, Baidoo L, Kip KE, Sepulveda AR, Pesci M, Harrison J, Plevy SE. Infliximab prevents crohn’s disease recurrence after ileal resection. Gastroenterology. 2009;136:441–50.
Riss S, Schuster I, Papay P, Mittlbock M, Stift A. Repeat intestinal resections increase the risk of recurrence of crohn’s disease. Dis Colon Rectum. 2013;56:881–7.
Riss S, Schuster I, Papay P, Herbst F, Mittlbock M, Chitsabesan P, Stift A. Surgical recurrence after primary ileocolic resection for crohn’s disease. Tech Coloproctol. 2014;18:365–71.
Walters TD, Steinhart AH, Bernstein CN, Tremaine W, McKenzie M, Wolff BG, McLeod RS. Validating crohn’s disease activity indices for use in assessing postoperative recurrence. Inflamm Bowel Dis. 2011;17:1547–56.
Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The montreal classification of inflammatory bowel disease: Controversies, consensus, and implications. Gut. 2006;55:749–53.
Clavien PA, Barkun J, Oliveira ML de, Vauthey JN, Dindo D, Schulick RD, Santibanes E de, Pekolj J, Slankamenac K, Bassi C, Graf R, Vonlanthen R, Padbury R, Cameron JL, Makuuchi M. The clavien-dindo classification of surgical complications: Five-year experience. Ann Surg. 2009;250:187–96.
Waugh N, Cummins E, Royle P, Kandala NB, Shyangdan D, Arasaradnam R, Clar C, Johnston R. Faecal calprotectin testing for differentiating amongst inflammatory and non-inflammatory bowel diseases: Systematic review and economic evaluation. Health Technol Assess. 2013;17(xv–xix):1–211.
Bellinger J, Munoz-Bongrand N, Pariente B, Baudry C, Chirica M, Gornet JM, Allez M, Cattan P. Endoscopic and clinical recurrences after laparoscopic or open ileocolic resection in crohn’s disease. J Laparoendosc Adv Surg Tech A. 2014;24:617–22.
Yoshida EM. The crohn’s disease activity index, its derivatives and the inflammatory bowel disease questionnaire: A review of instruments to assess crohn’s disease. Can J Gastroenterol. 1999;13:65–73.
Welsch T, Hinz U, Loffler T, Muth G, Herfarth C, Schmidt J, Kienle P. Early re-laparotomy for post-operative complications is a significant risk factor for recurrence after ileocaecal resection for crohn’s disease. Int J Colorectal Dis. 2007;22:1043–9.
Wolters FL, Russel MG, Sijbrandij J, Ambergen T, Odes S, Riis L, Langholz E, Politi P, Qasim A, Koutroubakis I, Tsianos E, Vermeire S, Freitas J, Zeijl G van, Hoie O, Bernklev T, Beltrami M, Rodriguez D, Stockbrugger RW, Moum B. Phenotype at diagnosis predicts recurrence rates in crohn’s disease. Gut. 2006;55:1124–30.
Vester-Andersen MK, Prosberg MV, Jess T, Andersson M, Bengtsson BG, Blixt T, Munkholm P, Bendtsen F, Vind I. Disease course and surgery rates in inflammatory bowel disease: A population-based, 7‑year follow-up study in the era of immunomodulating therapy. Am J Gastroenterol. 2014;109:705–14.
Henriksen M, Jahnsen J, Lygren I, Aadland E, Schulz T, Vatn MH, Moum B, Ibsen Study G. Clinical course in crohn’s disease: Results of a five-year population-based follow-up study (the ibsen study). Scand J Gastroenterol. 2007;42:602–10.
Mowat C, Cole A, Windsor A, Ahmad T, Arnott I, Driscoll R, Mitton S, Orchard T, Rutter M, Younge L, Lees C, Ho GT, Satsangi J, Bloom S, Gastroenterology IBDSotBSo. Guidelines for the management of inflammatory bowel disease in adults. Gut. 2011;60:571–607.
Munkholm P, Langholz E, Davidsen M, Binder V. Frequency of glucocorticoid resistance and dependency in crohn’s disease. Gut. 1994;35:360–2.
Ford AC, Khan KJ, Talley NJ, Moayyedi P. 5‑aminosalicylates prevent relapse of crohn’s disease after surgically induced remission: Systematic review and meta-analysis. Am J Gastroenterol. 2011;106:413–20.
Schwartz M, Regueiro M. Prevention and treatment of postoperative crohn’s disease recurrence: An update for a new decade. Curr Gastroenterol Rep. 2011;13:95–100.
Moran GW, Dubeau MF, Kaplan GG, Yang H, Seow CH, Fedorak RN, Dieleman LA, Barkema HW, Ghosh S, Panaccione R, Alberta Inflammatory Bowel Disease C. Phenotypic features of crohn’s disease associated with failure of medical treatment. Clin Gastroenterol Hepatol. 2014;12(434–42):e431.
Peyrin-Biroulet L. Tumor necrosis factor inhibitors for inflammatory bowel disease. N Engl J Med. 2013;369:2561.
Tursi A, Elisei W, Picchio M, Zampaletta C, Pelecca G, Faggiani R, Brandimarte G. Comparison of the effectiveness of infliximab and adalimumab in preventing postoperative recurrence in patients with crohn’s disease: An open-label, pilot study. Tech Coloproctol. 2014;18:1041–6.
Orlando A, Mocciaro F, Renna S, Scimeca D, Rispo A, Lia Scribano M, Testa A, Aratari A, Bossa F, Tambasco R, Angelucci E, Onali S, Cappello M, Fries W, D’Inca R, Martinato M, Castiglione F, Papi C, Annese V, Gionchetti P, Rizzello F, Vernia P, Biancone L, Kohn A, Cottone M. Early post-operative endoscopic recurrence in crohn’s disease patients: Data from an italian group for the study of inflammatory bowel disease (ig-ibd) study on a large prospective multicenter cohort. J Crohns Colitis. 2014;8:1217–21.
De Cruz P, Kamm MA, Hamilton AL, Ritchie KJ, Krejany EO, Gorelik A, Liew D, Prideaux L, Lawrance IC, Andrews JM, Bampton PA, Gibson PR, Sparrow M, Leong RW, Florin TH, Gearry RB, Radford-Smith G, Macrae FA, Debinski H, Selby W, Kronborg I, Johnston MJ, Woods R, Elliott PR, Bell SJ, Brown SJ, Connell WR, Desmond PV. Crohn’s disease management after intestinal resection: A randomised trial. Lancet. 2015;385:1406–17.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
H. Ribbing Wilén, P.-O. Nyström, L. Törkvist, and J. Blom declare that they have no competing interests.
Ethical standards
The accompanying manuscript does not include studies on humans or animals.
Rights and permissions
About this article

Cite this article
Ribbing Wilén, H., Nyström, PO., Törkvist, L. et al. Clinical and inflammatory response to first ileocolic resection for Crohn’s disease. Eur Surg 48, 209–214 (2016). https://doi.org/10.1007/s10353-016-0426-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10353-016-0426-0