Abstract
Purpose
To identify morphologic features of isolated cervical spine facet fractures that can reliably differentiate AOSpine F1 and F2 injuries.
Materials and methods
Retrospective review of cervical spine CTs on all patients who sustained isolated cervical fractures of the facets presenting to our level 1 trauma center from August 2012 through December 2015. CTs were reviewed for facet fracture characteristics and AOSpine facet fracture classification. Association between facet fracture characteristics and AOSpine classification was assessed through multivariable logistic regression models.
Results
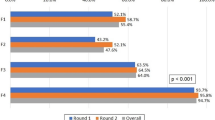
Fifty-six patients with cervical spine fractures isolated to the facets were included in the study. The mean age was 36 (range 9–90) years with 55.4% (n = 31) males. A significant correlation was found between subtype F1 and subtype F2 in laterality (left- or right-sided) (p = 0.004), interfacetal fracture involvement (p < 0.0001), transverse process involvement (p < 0.001), displacement of fracture fragment (p < 0.001), comminution of fracture (p < 0.0001), and vertebral arch disruption (p = 0.001). After multivariable analysis, left side laterality (p = 0.03), transverse process involvement (p = 0.01), and fracture comminution (p = 0.003) were associated with F2 fractures.
Conclusion
Facet fractures with transverse process involvement or comminution have a higher probability of being an F2 fracture. These characteristics may be helpful when categorizing facet fractures using the AOSpine classification.




Similar content being viewed by others


References
Lorenz B, Jörg B (1996) Die Technik Der Knochenbruchbehandlung. Maudrich
Urrutia J, Zamora T, Yurac R, Campos M, Palma J, Mobarec S, Prada C (2017) An independent inter- and intraobserver agreement evaluation of the AOSpine subaxial cervical spine injury classification system. Spine (Phila Pa 1976) 42(5):298–303
Vaccaro AR, Koerner JD, Radcliff KE, Oner FC, Reinhold M, Schnake KJ, Kandziora F, Fehlings MG, Dvorak MF, Aarabi B, Rajasekaran S, Schroeder GD, Kepler CK, Vialle LR (2016) AOSpine subaxial cervical spine injury classification system. Eur Spine J 25(7):2173–2184
Holdsworth F (1970) Fractures, dislocations, and fracture-dislocations of the spine. J Bone Joint Surg Am 52(8):1534–1551
Allen BL Jr, Ferguson RL, Lehmann TR, O'Brien RP (1982) A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine (Phila Pa 1976) 7(1):1–27
Aebi M, Nazarian S (1987) Classification of injuries of the cervical spine. Orthopade. 16(1):27–36
Vaccaro AR, Hulbert RJ, Patel AA, Fisher C, Dvorak M, Lehman RA Jr, et al. The subaxial cervical spine injury classification system: a novel approach to recognize the importance of morphology, neurology, and integrity of the disco-ligamentous complex. Spine (Phila Pa 1976) 2007;32(21):2365–2374
Stone AT, Bransford RJ, Lee MJ, Vilela MD, Bellabarba C, Anderson PA, Agel J (2010) Reliability of classification systems for subaxial cervical injuries. Evid Based Spine Care J 1(3):19–26
van Middendorp JJ, Audigé L, Bartels RH, Bolger C, Deverall H, Dhoke P, Diekerhof CH, Govaert GAM, Guimerá V, Koller H, Morris SAC, Setiobudi T, Hosman AJF (2013) The subaxial cervical spine injury classification system: an external agreement validation study. Spine J 13(9):1055–1063
Harris JH Jr, Edeiken-Monroe B, Kopaniky DR. A practical classification of acute cervical spine injuries. Orthop Clin North Am 1986;17(1):15–30
Schnake KJ, Schroeder GD, Vaccaro AR, Oner C (2017) AOSpine classification systems (subaxial, thoracolumbar). J Orthop Trauma 31(Suppl 4):S14–S23
Silva OT, Sabba MF, Lira HI, Ghizoni E, Tedeschi H, Patel AA, Joaquim AF (2016) Evaluation of the reliability and validity of the newer AOSpine subaxial cervical injury classification (C-3 to C-7). J Neurosurg Spine 25(3):303–308
Bono CM, Schoenfeld A, Rampersaud R, Levi A, Grauer J, Arnold P, Fehlings M, Dvorak M, Vaccaro AR (20111) Reproducibility of radiographic measurements for subaxial cervical spine trauma. Spine (Phila Pa 1976) 36(17):1374–1379
Spector LR, Kim DH, Affonso J, Albert TJ, Hilibrand AS, Vaccaro AR (2006) Use of computed tomography to predict failure of nonoperative treatment of unilateral facet fractures of the cervical spine. Spine (Phila Pa 1976) 31(24):2827–2835
van Eck CF, Fourman MS, Abtahi AM, Alarcon L, Donaldson WF, Lee JY (2017) Risk factors for failure of nonoperative treatment for unilateral cervical facet fractures. Asian Spine J 11(3):356–364
Leucht P, Fischer K, Muhr G, Mueller EJ (2009) Epidemiology of traumatic spine fractures. Injury. 40(2):166–172
Smith KM, Cummings P (2004) Passenger seating position and the risk of passenger death or injury in traffic crashes. Accid Anal Prev 36(2):257–260
Smith KM, Cummings P (2006) Passenger seating position and the risk of passenger death in traffic crashes: a matched cohort study. Inj Prev 12(2):83–86
McConnell EJ, Macbeth GA (1997) Common carotid artery and tracheal injury from shoulder strap seat belt. J Trauma 43(1):150–152
Harbison JM, Page MP (2010) Submandibular gland injury and delayed airway compromise caused by a seat belt. Am J Otolaryngol 31(3):209–211
Rozycki GS, Tremblay L, Feliciano DV, Tchorz K, Hattaway A, Fountain J, Pettitt BJ (2002) A prospective study for the detection of vascular injury in adult and pediatric patients with cervicothoracic seat belt signs. J Trauma 52(4):618–623 discussion 623-4
Urrutia J, Zamora T, Campos M, Yurac R, Palma J, Mobarec S, Prada C (2016) A comparative agreement evaluation of two subaxial cervical spine injury classification systems: the AOSpine and the Allen and Ferguson schemes. Eur Spine J 25(7):2185–2192
Acknowledgments
-
1.
Memorial Hospital System in Houston.
-
2.
We acknowledge the support provided by the Biostatistics/Epidemiology/Research Design (BERD) component of the Center for Clinical and Translational Sciences (CCTS) for this project. CCTS is mainly funded by a grant (UL1 TR000371) from the National Center for Advancing Translational Sciences (NCATS), awarded to University of Texas Health Science Center at Houston.
-
3.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NCATS.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix A
Appendix A
In the AOSpine subaxial cervical spine injury classification, injuries are classified based on morphology, facet injury, neurologic injury, and a small set of disease modifiers. Morphology is divided into three categories with each category assigned a letter classification: compression (A), tension band (B), and translation injuries (C). Compression injuries are further divided into five subtypes (A0–A4). A0 injuries are injuries without fracture (e.g., traumatic disc herniation) or minor fractures (e.g. spinous process or lamina fracture). A1 fractures are fractures through a single end plate without involvement of the posterior vertebral body cortex. A2 fractures are split fractures of the vertebral body involving both end plates without involvement of the posterior wall. A3 fractures are incomplete burst fractures involving a single end plate along with the posterior vertebral body cortex. A4 fractures are complete burst fractures involving both end plates along with the posterior vertebral body cortex. Tension band injuries are divided into three subtypes (B1–B3). B1 injuries are purely bony distraction injuries through the posterior elements. B2 injuries are distraction injuries through the posterior spine resulting in soft tissue disruption with or without accompanying bony injury. B3 injuries are all anterior distraction injury whether soft tissue or bony. There are no subcategories of translational injuries

Facet fractures are divided into four subtypes (F1–F4). F1 injuries are stable facet fractures, defined as fractures measuring less than 1 cm in length or less than 40% of the total lateral mass. F2 injuries are potentially unstable facet fracture, defined as fractures measuring more than 1 cm in length or more than 40% of the total lateral mass. F3 injuries are pedicolaminar fractures comprised of a combined fracture through the pedicle and ipsilateral lamina resulting in a free-floating lateral mass. F4 injuries are dislocated or perched facets regardless of whether a fracture is present. When classifying fractures, the right side facet fracture is described before the left facet. If both facet have the same grade of injury, the abbreviation “BL” is used.

Neurologic status is divided into six categories (N0–NX). N0 denotes a neurologically intact patient. N1 indicates a transient neurologic deficit. N2 represents a radiculopathy. Incomplete cord injuries are defined as N3, and N4 represents a complete cord injury. NX is used to describe patients in which neurologic status cannot be assessed. A modifier of “+” is added to denote continued spinal cord compression.
There are four potential clinical modifiers recognized in the AOSpine classification (M1–M4). M1 represents a posterior ligament complex injury without complete disruption (i.e., a B2-type injury without complete tearing of ligaments). M2 designates a critical disc herniation. M3 indicates a disease process that results in stiffening of the axial skeleton (e.g., diffuse idiopathic skeletal hyperostosis). M4 represents a vertebral artery injury.
Using the AOSpine classification system, complex clinical scenarios can be succinctly summarized as a short string of letters and numbers. For example, a patient with ankylosing spondylitis presenting with a hyperextension injury at C4–C5 resulting in right facet chip fracture, free-floating left facet, and transient upper extremity paresthesia can be simply classified as C4–C5:B3 (F1, F3, N1, M3) using the AOSpine system.
Rights and permissions
About this article

Cite this article
Jenjitranant, P., Beckmann, N.M., Cai, C. et al. There has to be an easier way: facet fracture characteristics that reliably differentiate AOSpine F1 and F2 injuries. Emerg Radiol 26, 391–399 (2019). https://doi.org/10.1007/s10140-019-01684-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-019-01684-1