
Abstract
Objectives
Aggregatibacter actinomycetemcomitans strains of serotype b and with a deletion of 530 bp in the promoter region of the leukotoxin gene (JP2 clone) are known to be associated with severe periodontitis. Our study was aimed to detect virulence genes of A. actinomycetemcomitans strains obtained from patients living in four German cities with different proportions of immigrants.
Material and methods
Samples were obtained from severe periodontitis patients in Frankfurt, Hamburg, Leipzig, and Jena. Those being tested positive for A. actinomycetemcomitans were analyzed for serotypes, deletion in the promoter region of the leukotoxin gene, presence of cytolethal distending toxin encoding genes (cdtA, cdtB, and cdtC) and fibril gene1(flp-1).
Results
From all 99 A. actinomycetemcomitans-positive samples, the JP2 clone was found in two immigrants in Frankfurt. Seventy strains were tested positive for the cdtA, 52 for cdtB, and 92 for cdtC and flp-1 genes. Twenty-five strains belonged to serotype a, 22 to serotype b, 21 to serotype c, 31 to the others or could not be serotyped, respectively. The distribution of the serotypes differed between the cities. Further, differences regarding the serotypes were also significant between natives and immigrants.
Conclusions
The JP2 clone is not spread within the Caucasian inhabitants in German cities. The serotypes distribution seems to be influenced by the numbers of immigrants in the cities.
Clinical Relevance
Patients originated from North Africa should be especially screened for the presence of the deletion in the ltx promoter region.
Similar content being viewed by others

Introduction
Periodontitis is an inflammatory disease affecting supporting tissues of the teeth. The prevalence of the disease was found to be up to 90% in Germany [1]. Among others such as Porphyromonas gingivalis and Tannerella forsythia, Aggregatibacter (formerly Actinobacillus) actinomycetemcomitans has been described as a powerful periodontopathogenic bacterial species [2]. It is acknowledged that A. actinomycetemcomitans strains affecting periodontitis patients vary significantly. Six different serotypes are described with differences in the structure of their lipopolysaccharides [3–5]. In general, serotype b is thought to be associated particularly with periodontal disease [6].
A. actinomycetemcomitans expresses many virulence factors [7]. It produces at least two toxins, a leukotoxin (LtxA) being a repeats-in-toxin (RTX) and a cytolethal distending toxin (Cdt). The leukotoxin affects polymorphonuclear neutrophiles, monocytes, and lymphocytes via binding to human leukocyte function-associated antigen-1 [8]. For the full activity of the leukotoxin, e.g., for the lysis of human leukocytes in vitro, the intracellular calcium level has to be increased by the leukotoxin [9]. At the beginning of the 1990s, in highly toxic strains (JP2 clone) of A. actinomycetemcomitans, a deletion of a 530-bp domain in the ltx promoter region was detected [10]. A high prevalence of these strains has been found in Morocco [11].
The cytolethal-distending toxin-encoding gene locus was found in a polymorphic region of the chromosome of A. actinomycetemcomitans and described to be similar to the genes cdtA, cdtB, and cdtC of Escherichia coli strains and Haemophilus ducreyi, respectively [12]. The cytolethal distending toxin acts as an immunosuppressive factor. It is capable to arrest the cell cycle in the G0/G1 or G2/M phase, promotes apoptosis, and stimulates the cytokine secretion of lymphocytes [13–15]. The activity is heavily increased when CdtA and CdtC are present [16]. CdtB, in contact with a subunit formed by CdtA and CdtC, acts as a functional toxin unit on the cell surface [15, 17]. Mutations in the cdtA gene are also known [18].
In addition to that, different virulence genes associated with adhesion of A. actinomycetemcomitans on host cells and solid surfaces are described. The species colonizes the oral cavity and probably forms also tenacious biofilms as seen in vitro on surfaces of glass and plastic or on saliva-coated hydroxyapatite [19]. The adherence on surfaces as well as the biofilm formation is mediated by fibril-associated protein (Flp) pili. The biogenesis of these Flp pili is encoded at the tad (tight adherence) locus of A. actinomycetemcomitans [20]. The flp-1 gene is one of 14 genes at the tad locus [21]. Mutations of the flp-1 gene subfamily are related to reduced adherence of A. actinomycetemcomitans due to short and unbundled pili [22].
The study was conducted to determine the presence of different virulence genes within A. actinomycetemcomitans strains in periodontitis patients living in four cities in Germany. Two of the four cities are located in the new federal states where a lower percentage of immigrants within citizens is common.
Materials and methods
Subject recruitment
Subjects with severe periodontitis and being tested positive for A. actinomycetemcomitans were recruited from patients of the Departments of Periodontology at the Universities of Frankfurt, Hamburg, Jena, and Leipzig over a period of 6 months in 2009. The patients were diagnosed according to the recent recommendation of the American Academy of Periodontology [23]. Severe periodontitis was diagnosed as an attachment loss of ≥5 mm at at least five sites, in different quadrants. Attachment loss and probing pocket depths were measured with a periodontal probe (PCP-UNC 15, Hu Friedy, Leimen, Germany) at six sites per tooth. Bleeding on probing was calculated as the percentage of positive sites per subject. Oral hygiene was recorded by using the plaque index described by O’Leary et al. [24]. Both indices were recorded and not further processed.
Patients with antibiotic therapy within the last 6 months or being pregnant or lactating females were excluded. In addition to that, the ethnic origin of the included subjects was registered. Ethical approval was obtained from the local ethics committees of the Universities of Jena, Frankfurt, Hamburg, and Leipzig. Written informed consent was obtained from each subject prior to participation.
Sample collection
For sampling, the deepest pocket in every quadrant was selected. Without removing supragingival plaque [25], the test site was air-dried and kept dry using cotton rolls. Sterile paper points were inserted into the selected periodontal pockets for 10 s to obtain subgingival plaque. If more than one site had the appropriate probing depth, subgingival plaque was sampled from those sites with signs of active inflammation, i.e., bleeding on probing, suppuration, and/or radiographic evidences of bone loss. Samples from four different pockets per patient were pooled in the transport vials and sent to the laboratory, where they were stored at −20°C until analyzed by nucleic acid-based methods.
Microflora
The DNA was extracted from the paper points using a DNA extraction system (A&A Biotechnology, Gdynia, Poland) according to the manufacturer's recommendations. First, the result for the presence of A. actinomycetemcomitans was confirmed by using polymerase chain reaction (PCR) which was carried out using a real-time rotary analyzer (RotorGene 2000; Corbett Research, Sydney, Australia). The primers for A. actinomycetemcomitans [26] were designed as described before. The PCR amplification was carried out in a reaction volume of 25 μl consisting of 2.5-μl template DNA and 22.5 μl of reaction mixture composed of 2.5 μl 10× PCR buffer, 2.75 mM MgCl2, 0.2 mM nucleotides, 0.5 μM primer each, 10−4 SybrGreen, and 1.5 U taq polymerase (Fermentas Life Science, St. Leon-Rot, Germany). Negative and positive controls were included in each batch of specimens. The positive control consisted of genomic DNA of A. actinomycetemcomitans Y4 strain; the negative control was dH2O. The cycling conditions comprised an initial denaturation step at 95°C for 5 min, followed by 45 cycles at 95°C for 15 s, at 58°C for 20 s, and at 72°C for 20 s.
PCR detection of serotypes, leukotoxin, cytolethal distending toxin, and fimbriae gene
In all samples tested positive for A. actinomycetemcomitans, additional PCRs were performed. First, each of the six PCRs was performed to differentiate the serotypes (a through f). Then, the samples were tested for the presence of ltx gene and screened for the 530-bp deletion, characterizing the highly leukotoxic clone, by PCR. Here, primers were used as recently described [11]. In some cases, the PCR products were difficult to analyze due to of smears on the gels; for that reason, the primers had been selected using GenBank. As controls, JP2, as a highly leukotoxic strain, and ATCC 33384, as a strain without deletion in the ltx promoter region, were used. The PCRs for detecting the three genes of the cytolethal distending toxin (cdtA, cdtB, and cdtC) as well as for detecting the flp-1 gene used the primers described recently [27, 28]. All primers and annealing temperatures are presented in Table 1.
Using a thermal cycler (Mastercycler proS; Eppendorf, Hamburg, Germany), all amplifications were carried out in 25-μl volumes, each containing 0.5 pmol primer, 0.2 mM deoxynucleoside triphosphates, onefold reaction buffer with 2.5 mM MgCl2, 1 U native Taq polymerase (Fermentas Life Science), and 2.5-μl template DNA. The PCR was performed with an initial denaturation at 94°C for 3 min for 35 cycles, with one cycle consisting of a denaturation at 94°C for 15 s, annealing at different temperatures according to the melting temperatures of the selected primers (Table 1), a polymerization at 72°C for 30 s, and a final extension at 72°C for 2 min. The amplified PCR products were analyzed by electrophoresis on a 1.5% agarose gel.
Statistical analysis
The comparisons between the different cities as well as between natives and immigrants were made by using the χ2 test.
Results
Subjects
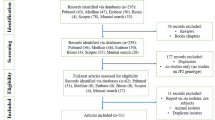
All patients screened and eligible for the study agreed to participate. The included patients are characterized in Table 2. In total, 52 patients suffered from aggressive periodontitis, 46 from chronic periodontitis, and 1 patient from a periodontitis as a manifestation of a systemic disease (Papillon–Lefèvre syndrome). Immigrants were included in Frankfurt and Hamburg; in Jena and Leipzig, all patients were natives.
Serotypes
All six serotypes were detected. Twenty-five strains belonged to serotype a, 22 to serotype b, 21 to serotype c, 24 to the other known serotypes, and in 7 samples no serotype was identified. Different percentages of serotypes were found in the four cities (p < 0.001). Thus, serotype a was detected in 44.4% of the samples from Leipzig but was not present in Frankfurt. Differences regarding the serotypes were also significant between natives and immigrants. Only in 2 of the 21 immigrants (9.5% originating from Iran) serotype a was detected, whereas 23 (29.5%) A. actinomycetemcomitans strains isolated from natives were serotype a. Serotypes b and c were present in 14 (17.9%) and 11 (14.1%) of the 78 natives' and in 8 (38.1%) and 10 (47.6%) of the 21 immigrants' samples (Table 3).
Deletion of the promoter region of leukotoxin gene
All strains exhibited the leukotoxin gene (i.e., lktA). The 530-bp deletion in the promoter region of the ltx operon was only found in two immigrants from North Africa who have lived in Frankfurt for 28 years and 11.5 years, respectively. Both patients had severe periodontitis characterized by a mean periodontal pocket depth of >10 mm at the sampling sites.
Cytolethal distending toxin genes
From 99 strains, 70 were tested positive for the cdtA, 52 for cdtB, and 92 for cdtC genes. The presence of cdtB and cdtC differed significantly between the cities (cdtB, p < 0.001; cdtC, p = 0.041). All three genes of the cdt operon are expressed in 45.5% of the samples; here the highest prevalence was seen in Hamburg, the lowest in Leipzig (difference between the cities, p < 0.001). The CdtB encoding gene as well as all three genes in a total were more present in A. actinomycetemcomitans positive samples originated from immigrants (cdtB, p = 0.013; cdtABC, p = 0.025; Table 4).
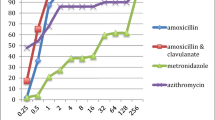
The cdtA and cdtC genes were found in all serotype b samples. Further all serotype d samples were tested positive for cdtA; contrary, cdtB was missing there (differences between serotypes—cdtA, p = 0.007; cdtB, p = 0.009; cdtC, p = 0.009; cdtABC, p = 0.003; Fig. 1).

Presence of genes of the cytolethal distending toxin (cdt) according to the serotypes of A. actinomycetemcomitans within the subgingival plaque samples
Fimbriae gene
The flp-1 gene was found in 92 (92.9%) of all cases. The gene was detectable in all samples from Frankfurt. In all these patients the flp-1 gene was found (Table 4). The flp-1 gene was partially missing in serotype e and f as well as in non-serotypeable samples, but the detection failed in only 1 of the 25 serotype a samples and in none of the b and c samples (differences between serotypes, p = 0.002; Fig. 2).

Presence of the fimbriae gene (flp-1) according to the serotypes of A. actinomycetemcomitans within the subgingival plaque samples
Clinical diagnosis of periodontitis and presence of genes
The patient diagnosed with Papillon–Lefèvre syndrome (serotype c, flp-1 negative, and cdtB negative) was not included in an analysis comparing aggressive and chronic periodontitis patients. Serotype distribution differed between chronic and aggressive periodontitis patients (p = 0.005). In aggressive periodontitis, 31 of the 52 strains (59.6%) belonged to serotype b or c (32.7% b, 26.9% c), whereas in chronic periodontitis only 11 of the 46 strains (23.9%) were serotyped as b (10.9%) or c (13.0%).
All three cdt genes (cdtABC) were detected in 33 of 52 (63.5%) strains originated from aggressive periodontitis and only in 12 of the 46 (26.1%) A. actinomycetemcomitans-positive chronic periodontitis samples (p = 0.002). The presence of the flp-1 gene did not differ between aggressive and chronic periodontitis patients.
Discussion
A. actinomycetemcomitans-positive samples obtained from periodontitis patients living in four cities in Germany with different proportions of immigrants have been analyzed by nucleic acid-based methods for presence of virulence genes of that bacterial species. Only nucleic acid-based methods were finally chosen. Initially cultivation was tried but failed in part due to issues concerning the transport of the samples. It is the first study comparing A. actinomycetemcomitans strains between cities in a closed area within Central Europe. The study population was representative of each of the participating university departments. Patients with severe periodontitis and tested positive for A. actinomycetemcomitans were studied. Their median age was between 33 and 49 years in the four German cities. The classification of periodontal diseases introduced in 1999 removed the age dependency as a primary criterion [23]. The discrimination between aggressive and chronic periodontitis was secondary in our study. A. actinomycetemcomitans was prevalent in both forms of periodontitis. This is not in contrast to other studies. Those described a high prevalence and percentage of A. actinomycetemcomitans in aggressive but also in chronic periodontitis patients [30]. The study did not focus on the prevalence of A. actinomycetemcomitans in the population of the studied cities. Our results suggest disease-related differences of the prevalence of A. actinomycetemcomitans between the cities. Two cities (Hamburg and Frankfurt) are located in the old federal states and the other two (Jena and Leipzig) in the new federal states of Germany. It is known that the percentage of immigrants living in these cities is different. In 2009, according to a publicly available data, the percentages of foreigners were 12–13% in the German federal states Hamburg and Hesse (Frankfurt) compared to about 2% in Saxonia (Leipzig) and Thuringia (Jena); the percentage of people with migration background is 39.5% in Frankfurt which is among the highest in Germany [29].
In this study, the distribution of genotypes of A. actinomycytemcomitans was found not to be uniform in the four included cities. In only two samples, obtained from North Africans (19 and 29 years old) who have lived in Frankfurt for many years, the deletion of a 530-bp domain in the ltx promoter region was detected. This supports former reports of an ethnic tropism of this clone. The JP2 clone is known to be strongly associated with aggressive periodontitis in North and West Africa [30]. Like in other studies [4, 31–33], highly leukotoxic JP2 clones of A. actinomycetemcomitans with the 530 bp in deletion in the ltx promoter region could not be isolated from the natives. Only one description of JP2 clones in two individuals, one 33 and one 62-year-old female, within the Caucasian family was published [34]; thus in Caucasions the JP2 clone may occur in older people. Also within Asian populations, studies failed to detect A. actinomycetemcomitans with the JP2-like promoter of the ltx operon in patients with moderate to advanced periodontitis [35, 36]. Different data were reported from Brazil. Cortelli et al. [37] detected the highly leukotoxic JP2-like ltx promoter pattern in 31% of A. actinomycetemcomitans isolates, whereas Vieira et al. [38] found only non-JP2 clones in plaque and saliva samples from Brazilian Indians. In the study of Cortelli et al. [37], the ethnicity of the patients was not mentioned, but the population living in Brazil has 45% inhabitants with African background [39].
A. actinomycetemcomitans serotypes a, b, and c were the predominant serotypes in Germany, more than two thirds of the detected strains belonged to these serotypes. These serotypes are globally dominant as reported from Taiwan [40], the USA [4], and Greece [33]. Nevertheless, the distribution of serotypes depends on geographic regions. In Asia serotype c is more often detectable than serotype b, in Europe the prevalence is vice versa in periodontitis patients [41]. The serotypes b and c were most prevalent in Frankfurt associated with the high percentage of immigrants included from this city in the study. In addition, the clinical diagnosis of periodontitis may be of importance; both serotypes were more often detectable in aggressive periodontitis patients than in chronic periodontitis patients. Serotype a was dominant in Leipzig. This serotype occurred more often than other serotypes in a population of untreated periodontitis patients in Greece [33]. As in other studies [28, 36], the prevalence of the other serotypes (especially d) was much lower, in Leipzig only seven strains were detected. Further, a few strains were not typeable to serotypes a–f. Some of these may belong to the recently described serotype g [42], but we have not examined that. Only one serotype was found per patient which confirms studies published some years ago [43, 44]. Other authors describe different serotypes within one patient [36, 40]. In the present study, only selected deep pockets were used, and probably not all strains colonizing the oral cavity were included.
In about half of our samples, all three cdtABC genes were detected. cdtB gene presence is essential for functional Cdt [27]. Again, a difference between the cities in the old and the new German federal states was obvious. In Frankfurt and Hamburg, these numbers were much higher than in Jena and Leipzig. In Jena and Leipzig, immigrants did not contribute to the study. The percentage of samples positive for all three genes was only in Hamburg close to former studies [45, 46]. Serotypes a, b, and c strains showed the highest frequency of detections of all cdt genes, whereas cdtB was not found in any of the serotype d samples, which suggests a lower virulence of that serotype. In Leipzig the percentage of included cases with chronic periodontitis was higher than in other cities. In chronic periodontitis, a lower percentage of samples being positive for all cdt genes was found in comparison to aggressive periodontitis. This is a contrast to recently published data where no differences in the cdt gene complex prevalence between patients with and without aggressive periodontitis were reported [47].
The flp1-gene plays a role for periodontal bone loss as well as for the immune response to A. actinomycetemcomitans in rats [48]. More than 90% of the strains investigated in this study have been tested positive for flp-1. Thus, our data reveal higher frequencies than those reported by others with 75–80% [28, 49]. All serotypes b, c, and d strains were positive for that gene, which generally confirms the results described before [28].
The different genotypes of A. actinomycetemcomitans are not evenly spread within a population. Even in a small geographic area, the genotype primarily depends on the ethnicity of the patient. In natives in Leipzig, more uncommon serotypes often associated with missing virulence genes were detected. Further analysis is needed to correlate microbiological findings and clinical data more detailed. In patients originating from North Africa, the JP2 clone is prevalent even after living in a European country for more than 10 years. Especially, these patients should be screened for the presence of deletion in the ltx promoter region to have an additional but important tool to assess the individual risk and to adjust the treatment on the individual level.
References
Holtfreter B, Schwahn C, Biffar R, Kocher T (2009) Epidemiology of periodontal diseases in the study of health in Pomerania. J Clin Periodontol 36:114–23
Henderson B, Ward JM (2000) Ready D (2010) Aggregatibacter (Actinobacillus) actinomycetemcomitans: a triple A* periodontopathogen? Periodontol 54:78–105
Saarela M, Asikainen S, Alaluusua S, Pyhala L, Lai CH, Jousimies-Somer H (1992) Frequency and stability of mono- or poly-infection by Actinobacillus actinomycetemcomitans serotypes a, b, c, d or e. Oral Microbiol Immunol 7:277–9
Kaplan JB, Schreiner HC, Furgang D, Fine DH (2002) Population structure and genetic diversity of Actinobacillus actinomycetemcomitans strains isolated from localized juvenile periodontitis patients. J Clin Microbiol 40:1181–7
Lakio L, Paju S, Alfthan G, Tiirola T, Asikainen S, Pussinen PJ (2003) Actinobacillus actinomycetemcomitans serotype d-specific antigen contains the O antigen of lipopolysaccharide. Infect Immun 71:5005–11
Socransky SS, Haffajee AD, Smith C, Dibart S (1991) Relation of counts of microbial species to clinical status at the sampled site. J Clin Periodontol 18:766–75
Kawamoto D, Ando ES, Longo PL, Nunes AC, Wikstrom M, Mayer MP (2009) Genetic diversity and toxic activity of Aggregatibacter actinomycetemcomitans isolates. Oral Microbiol Immunol 24:493–501
Kieba IR, Fong KP, Tang HY, Hoffman KE, Speicher DW, Klickstein LB, Lally ET (2007) Aggregatibacter actinomycetemcomitans leukotoxin requires beta-sheets 1 and 2 of the human CD11a beta-propeller for cytotoxicity. Cell Microbiol 9:2689–99
Balashova NV, Shah C, Patel JK, Megalla S, Kachlany SC (2009) Aggregatibacter actinomycetemcomitans LtxC is required for leukotoxin activity and initial interaction between toxin and host cells. Gene 443:42–7
Brogan JM, Lally ET, Poulsen K, Kilian M, Demuth DR (1994) Regulation of Actinobacillus actinomycetemcomitans leukotoxin expression: analysis of the promoter regions of leukotoxic and minimally leukotoxic strains. Infect Immun 62:501–8
Haubek D, Poulsen K, Westergaard J, Dahlen G, Kilian M (1996) Highly toxic clone of Actinobacillus actinomycetemcomitans in geographically widespread cases of juvenile periodontitis in adolescents of African origin. J Clin Microbiol 34:1576–8
Mayer MP, Bueno LC, Hansen EJ, DiRienzo JM (1999) Identification of a cytolethal distending toxin gene locus and features of a virulence-associated region in Actinobacillus actinomycetemcomitans. Infect Immun 67:1227–37
Akifusa S, Heywood W, Nair SP, Stenbeck G, Henderson B (2005) Mechanism of internalization of the cytolethal distending toxin of Actinobacillus actinomycetemcomitans. Microbiology 151:1395–402
Oscarsson J, Karched M, Thay B, Chen C, Asikainen S (2008) Proinflammatory effect in whole blood by free soluble bacterial components released from planktonic and biofilm cells. BMC Microbiol 8:206
Shenker BJ, Besack D, McKay T, Pankoski L, Zekavat A, Demuth DR (2005) Induction of cell cycle arrest in lymphocytes by Actinobacillus actinomycetemcomitans cytolethal distending toxin requires three subunits for maximum activity. J Immunol 174:2228–34
Shenker BJ, Dlakic M, Walker LP, Besack D, Jaffe E, LaBelle E, Boesze-Battaglia K (2007) A novel mode of action for a microbial-derived immunotoxin: the cytolethal distending toxin subunit B exhibits phosphatidylinositol 3,4,5-triphosphate phosphatase activity. J Immunol 178:5099–108
Shenker BJ, Besack D, McKay T, Pankoski L, Zekavat A, Demuth DR (2004) Actinobacillus actinomycetemcomitans cytolethal distending toxin (Cdt): evidence that the holotoxin is composed of three subunits: CdtA, CdtB, and CdtC. J Immunol 172:410–7
Cao L, Volgina A, Huang CM, Korostoff J, DiRienzo JM (2005) Characterization of point mutations in the cdtA gene of the cytolethal distending toxin of Actinobacillus actinomycetemcomitans. Mol Microbiol 58:1303–21
Kaplan JB, Meyenhofer MF, Fine DH (2003) Biofilm growth and detachment of Actinobacillus actinomycetemcomitans. J Bacteriol 185:1399–404
Tomich M, Fine DH, Figurski DH (2006) The TadV protein of Actinobacillus actinomycetemcomitans is a novel aspartic acid prepilin peptidase required for maturation of the Flp1 pilin and TadE and TadF pseudopilins. J Bacteriol 188:6899–914
Planet PJ, Kachlany SC, Fine DH, DeSalle R, Figurski DH (2003) The widespread colonization island of Actinobacillus actinomycetemcomitans. Nat Genet 34:193–8
Kachlany SC, Planet PJ, Desalle R, Fine DH, Figurski DH, Kaplan JB (2001) flp-1, the first representative of a new pilin gene subfamily, is required for non-specific adherence of Actinobacillus actinomycetemcomitans. Mol Microbiol 40:542–54
Armitage GC (1999) Development of a classification system for periodontal diseases and conditions. Ann Periodontol 4:1–6
O'Leary TJ, Drake RB, Naylor JE (1972) The plaque control record. J Periodontol 43:38
Beikler T, Schnitzer S, Abdeen G, Ehmke B, Eisenacher M, Flemmig TF (2006) Sampling strategy for intraoral detection of periodontal pathogens before and following periodontal therapy. J Periodontol 77:1323–32
Tran SD, Rudney JD (1999) Improved multiplex PCR using conserved and species-specific 16S rRNA gene primers for simultaneous detection of Actinobacillus actinomycetemcomitans, Bacteroides forsythus, and Porphyromonas gingivalis. J Clin Microbiol 37:3504–8
Fabris AS, DiRienzo JM, Wikstrom M, Mayer MP (2002) Detection of cytolethal distending toxin activity and cdt genes in Actinobacillus actinomycetemcomitans isolates from geographically diverse populations. Oral Microbiol Immunol 17:231–8
Kaplan JB, Kokeguchi S, Murayama Y, Fine DH (2002) Sequence diversity in the major fimbrial subunit gene (flp-1) of Actinobacillus actinomycetemcomitans. Oral Microbiol Immunol 17:354–9
Federal Statistical Office G (2010) Available at http://www.destatis.de/jetspeed/portal/cms/Sites/destatis/Internet/DE/Navigation/Statistiken/Bevoelkerung/Bevoelkerung.psml
Haubek D, Ennibi OK, Poulsen K, Vaeth M, Poulsen S, Kilian M (2008) Risk of aggressive periodontitis in adolescent carriers of the JP2 clone of Aggregatibacter (Actinobacillus) actinomycetemcomitans in Morocco: a prospective longitudinal cohort study. Lancet 371:237–42
Macheleidt A, Muller HP, Eger T, Putzker M, Fuhrmann A, Zoller L (1999) Absence of an especially toxic clone among isolates of Actinobacillus actinomycetemcomitans recovered from army recruits. Clin Oral Investig 3:161–7
Fine DH, Markowitz K, Furgang D, Fairlie K, Ferrandiz J, Nasri C, McKiernan M, Gunsolley J (2007) Aggregatibacter actinomycetemcomitans and its relationship to initiation of localized aggressive periodontitis: longitudinal cohort study of initially healthy adolescents. J Clin Microbiol 45:3859–69
Sakellari D, Katsikari A, Slini T, Ioannidis I, Konstantinidis A, Arsenakis M (2011) Prevalence and distribution of Aggregatibacter actinomycetemcomitans serotypes and the JP2 clone in a Greek population. J Clin Periodontol 38:108–14
Claesson R, Lagervall M, Hoglund-Aberg C, Johansson A, Haubek D (2011) Detection of the highly leucotoxic JP2 clone of Aggregatibacter actinomycetemcomitans in members of a Caucasian family living in Sweden. J Clin Periodontol 38:115–21
Tan KS, Woo CH, Ong G, Song KP (2001) Prevalence of Actinobacillus actinomycetemcomitans in an ethnic adult Chinese population. J Clin Periodontol 28:886–90
Mombelli A, Gmur R, Lang NP, Corbert E, Frey J (1999) Actinobacillus actinomycetemcomitans in Chinese adults. Serotype distribution and analysis of the leukotoxin gene promoter locus. J Clin Periodontol 26:505–10
Cortelli SC, Jorge AO, Cortelli JR, Jordan SF, Haraszthy VI (2003) Detection of highly and minimally leukotoxic Actinobacillus actinomycetemcomitans strains in patients with periodontal disease. Pesqui Odontol Bras 17:183–8
Vieira EM, Raslan SA, Wahasugui TC, Avila-Campos MJ, Marvulle V, Gaetti-Jardim Junior E (2009) Occurrence of Aggregatibacter actinomycetemcomitans in Brazilian Indians from Umutina Reservation, Mato Grosso, Brazil. J Appl Oral Sci 17:440–5
Factbook TW (2011) Available at https://www.cia.gov/library/publications/the-world-factbook/geos/br.html
Yang HW, Huang YF, Chan Y, Chou MY (2005) Relationship of Actinobacillus actinomycetemcomitans serotypes to periodontal condition: prevalence and proportions in subgingival plaque. Eur J Oral Sci 113:28–33
Kim TS, Frank P, Eickholz P, Eick S, Kim CK (2009) Serotypes of Aggregatibacter actinomycetemcomitans in patients with different ethnic backgrounds. J Periodontol 80:2020–7
Takada K, Saito M, Tsuzukibashi O, Kawashima Y, Ishida S, Hirasawa M (2010) Characterization of a new serotype g isolate of Aggregatibacter actinomycetemcomitans. Mol Oral Microbiol 25:200–6
Zambon JJ, Christersson LA, Slots J (1983) Actinobacillus actinomycetemcomitans in human periodontal disease. Prevalence in patient groups and distribution of biotypes and serotypes within families. J Periodontol 54:707–11
DiRienzo JM, Slots J (1990) Genetic approach to the study of epidemiology and pathogenesis of Actinobacillus actinomycetemcomitans in localized juvenile periodontitis. Arch Oral Biol 35(Suppl):79S–84S
Ahmed HJ, Svensson LA, Cope LD, Latimer JL, Hansen EJ, Ahlman K, Bayat-Turk J, Klamer D, Lagergard T (2001) Prevalence of cdtABC genes encoding cytolethal distending toxin among Haemophilus ducreyi and Actinobacillus actinomycetemcomitans strains. J Med Microbiol 50:860–4
Yamano R, Ohara M, Nishikubo S, Fujiwara T, Kawamoto T, Ueno Y, Komatsuzawa H, Okuda K, Kurihara H, Suginaka H, Oswald E, Tanne K, Sugai M (2003) Prevalence of cytolethal distending toxin production in periodontopathogenic bacteria. J Clin Microbiol 41:1391–8
Leung WK, Ngai VK, Yau JY, Cheung BP, Tsang PW, Corbet EF (2005) Characterization of Actinobacillus actinomycetemcomitans isolated from young Chinese aggressive periodontitis patients. J Periodontal Res 40:258–68
Schreiner HC, Sinatra K, Kaplan JB, Furgang D, Kachlany SC, Planet PJ, Perez BA, Figurski DH, Fine DH (2003) Tight-adherence genes of Actinobacillus actinomycetemcomitans are required for virulence in a rat model. Proc Natl Acad Sci U S A 100:7295–300
Wu YM, Yan J, Chen LL, Gu ZY (2007) Association between infection of different strains of Porphyromonas gingivalis and Actinobacillus actinomycetemcomitans in subgingival plaque and clinical parameters in chronic periodontitis. J Zhejiang Univ Sci B 8:121–31
Goncharoff P, Figurski DH, Stevens RH, Fine DH (1993) Identification of Actinobacillus actinomycetemcomitans: polymerase chain reaction amplification of lktA-specific sequences. Oral Microbiol Immunol 8:105–10
Kaplan JB, Perry MB, MacLean LL, Furgang D, Wilson ME, Fine DH (2001) Structural and genetic analyses of O polysaccharide from Actinobacillus actinomycetemcomitans serotype f. Infect Immun 69:5375–84
Acknowledgments
The authors wish to thank Claudia Ranke, Hanna Loester, and Christopher Buchmann for their valuable laboratory work. Further we are grateful to Rolf Claesson (University of Umeå, Sweden) for providing us with control strains of A. actinomycetemcomitans.
Conflict of interest
Most of the study was institutionally founded. Further, this study was supported by Hain Lifescience GmbH, Nehren, Germany. The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Holger Jentsch and Georg Cachovan contributed equally to this manuscript.
Rights and permissions
About this article
Cite this article
Jentsch, H., Cachovan, G., Guentsch, A. et al. Characterization of Aggregatibacter actinomycetemcomitans strains in periodontitis patients in Germany. Clin Oral Invest 16, 1589–1597 (2012). https://doi.org/10.1007/s00784-012-0672-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-012-0672-x