
Abstract
Background
Cervical spine injuries of variable severity are common among patients with an acute traumatic brain injury (TBI). We hypothesised that TBI patients with positive head computed tomography (CT) scans would have a significantly higher risk of having an associated cervical spine fracture compared to patients with negative head CT scans.
Method
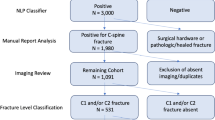
This widely generalisable retrospective sample was derived from 3,023 consecutive patients, who, due to an acute head injury (HI), underwent head CT at the Emergency Department of Tampere University Hospital (August 2010–July 2012). Medical records were reviewed to identify the individuals whose cervical spine was CT-imaged within 1 week after primary head CT due to a clinical suspicion of a cervical spine injury (CSI) (n = 1,091).
Results
Of the whole cranio-cervically CT-imaged sample (n = 1,091), 24.7% (n = 269) had an acute CT-positive TBI. Car accidents 22.4% (n = 244) and falls 47.8% (n = 521) were the most frequent injury mechanisms. On cervical CT, any type of fracture was found in 6.6% (n = 72) and dislocation and/or subluxation in 2.8% (n = 31) of the patients. The patients with acute traumatic intracranial lesions had significantly (p = 0.04; OR = 1.689) more cervical spine fractures (9.3%, n = 25) compared to head CT-negative patients (5.7%, n = 47). On an individual cervical column level, head CT positivity was especially related to C6 fractures (p = 0.031, OR = 2.769). Patients with cervical spine fractures (n = 72) had altogether 101 fractured vertebrae, which were most often C2 (22.8, n = 23), C7 (19.8%, n = 20) and C6 (16.8%, n = 17).
Conclusions
Head trauma patients with acute intracranial lesions on CT have a higher risk for cervical spine fractures in comparison to patients with a CT-negative head injury. Although statistically significant, the difference in fracture rate was small. However, based on these results, we suggest that cervical spine fractures should be acknowledged when treating CT-positive TBIs.

Similar content being viewed by others


References
Anderson PA, Muchow RD, Munoz A, Tontz WL, Resnick DK (2010) Clearance of the asymptomatic cervical spine: a meta-analysis. J Orthop Trauma 24:100–106
Bayless P, Ray VG (1989) Incidence of cervical spine injuries in association with blunt head trauma. Am J Emerg Med 7:139–142
Blackmore CC, Emerson SS, Mann FA, Koepsell TD (1999) Cervical spine imaging in patients with trauma: determination of fracture risk to optimize use. Radiology 211:759–765
Drainer EK, Graham CA, Munro PT (2003) Blunt cervical spine injuries in Scotland 1995–2000. Injury 34:330–333
Fujii T, Faul M, Sasser S (2013) Risk factors for cervical spine injury among patients with traumatic brain injury. J Emerg Trauma Shock 6:252–258
Gbaanador GB, Fruin AH, Taylon C (1986) Role of routine emergency cervical radiography in head trauma. Am J Surg 152:643–648
Goldberg W, Mueller C, Panacek E, Tigges S, Hoffman JR, Mower WR, NEXUS Group (2001) Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med 38:17–21
Hasler RM, Exadaktylos AK, Bouamra O, Benneker LM, Clancy M, Sieber R, Zimmermann H, Lecky F (2012) Epidemiology and predictors of cervical spine injury in adult major trauma patients: a multicenter cohort study. J Trauma Acute Care Surg 72:975–981
Hessmann MH, Hofmann A, Kreitner KF, Lott C, Rommens PM (2006) The benefit of multislice CT in the emergency room management of polytraumatized patients. Acta Chir Belg 106:500–507
Hills MW, Deane SA (1993) Head injury and facial injury: is there an increased risk of cervical spine injury? J Trauma 34:549–553, discussion 553–4
Hoffman JR, Wolfson AB, Todd K, Mower WR (1998) Selective cervical spine radiography in blunt trauma: methodology of the national emergency X-radiography utilization study (NEXUS). Ann Emerg Med 32:461–469
Holly LT, Kelly DF, Counelis GJ, Blinman T, McArthur DL, Cryer HG (2002) Cervical spine trauma associated with moderate and severe head injury: incidence, risk factors, and injury characteristics. J Neurosurg 96:285–291
Holm L, Cassidy JD, Carroll LJ, Borg J, Neurotrauma Task Force on Mild Traumatic Brain Injury of the WHO Collaborating Centre (2005) Summary of the WHO collaborating centre for neurotrauma task force on mild traumatic brain injury. J Rehabil Med 37:137–141
Ingebrigtsen T, Romner B, Kock-Jensen C (2000) Scandinavian guidelines for initial management of minimal, mild, and moderate head injuries. The scandinavian neurotrauma committee. J Trauma 48:760–766
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, Johansen M, Jones L, Krassioukov A, Mulcahey MJ, Schmidt-Read M, Waring W (2011) International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med 34:535–546
Linsenmaier U, Krotz M, Hauser H, Rock C, Rieger J, Bohndorf K, Pfeifer KJ, Reiser M (2002) Whole-body computed tomography in polytrauma: techniques and management. Eur Radiol 12:1728–1740
Mathews JD, Forsythe AV, Brady Z, Butler MW, Goergen SK, Byrnes GB, Giles GG, Wallace AB, Anderson PR, Guiver TA, McGale P, Cain TM, Dowty JG, Bickerstaffe AC, Darby SC (2013) Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians. BMJ 346:f2360
Michael DB, Guyot DR, Darmody WR (1989) Coincidence of head and cervical spine injury. J Neurotrauma 6:177–189
Milby AH, Halpern CH, Guo W, Stein SC (2008) Prevalence of cervical spinal injury in trauma. Neurosurg Focus 25:E10
Mulligan RP, Friedman JA, Mahabir RC (2010) A nationwide review of the associations among cervical spine injuries, head injuries, and facial fractures. J Trauma 68:587–592
Schmidt OI, Gahr RH, Gosse A, Heyde CE (2009) ATLS(R) and damage control in spine trauma. World J Emerg Surg 4:9
Schoenfeld AJ, Bono CM, McGuire KJ, Warholic N, Harris MB (2010) Computed tomography alone versus computed tomography and magnetic resonance imaging in the identification of occult injuries to the cervical spine: a meta-analysis. J Trauma 68:109–113, discussion 113–4
Soicher E, Demetriades D (1991) Cervical spine injuries in patients with head injuries. Br J Surg 78:1013–1014
Tian HL, Guo Y, Hu J, Rong BY, Wang G, Gao WW, Chen SW, Chen H (2009) Clinical characterization of comatose patients with cervical spine injury and traumatic brain injury. J Trauma 67:1305–1310
Vahldiek JL, Thieme S, Hamm B, Niehues SM (2016) Incidence of combined cranial and cervical spine injuries in patients with blunt minor trauma: are combined CT examinations of the head and cervical spine justified?. Acta Radiol. doi:10.1177/0284185116673120
Williams J, Jehle D, Cottington E, Shufflebarger C (1992) Head, facial, and clavicular trauma as a predictor of cervical-spine injury. Ann Emerg Med 21:719–722
Acknowledgements
The authors wish to thank nurse Anne Simi for her assistance in data collection.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organisation or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Funding
No funding was received for this work.
Ethical approval
For this type of study formal consent is not required.
Additional information
Comments
Analysing a large 2-year emergency room cohort retrospectively, the authors demonstrate that head injured patients with intracranial lesions on CT harbour an 1.7-fold increased risk of cervical fractures in comparison to CT-negative patients. The conclusion that cervical fractures should be acknowledged when treating CT-positive TBIs can obviously be supported and is kept in mind intuitively in general practice already. The study provides further proof for this concept. However, the risk difference of 9.3% versus 5.7% is too small to make a real difference in the ER. The c-spine clearance rules still have to be applied. Surprisingly, the rate of spinal cord injury was higher in the CT-negative cohort (1.5% vs 0.4%, i.e. 12 patients versus one single patient). It could be speculated that this may be due to central cord syndromes after minor falls in the elderly and is an interesting finding.
Claudius Thome
Tirol, Austria
An erratum to this article is available at http://dx.doi.org/10.1007/s00701-017-3156-6.
Rights and permissions
About this article

Cite this article
Thesleff, T., Kataja, A., Öhman, J. et al. Head injuries and the risk of concurrent cervical spine fractures. Acta Neurochir 159, 907–914 (2017). https://doi.org/10.1007/s00701-017-3133-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-017-3133-0