
Abstract
Background
Patients with Chiari malformation type 1 (CMI) often present with elevated pulsatile and static intracranial pressure (ICP). The preferred treatment of CMI, foramen magnum decompression (FMD), is assumed to normalise ICP and craniospinal pressure dissociation. In order to further explore the mechanisms behind FMD, the present study investigated whether or not pulsatile and static ICP normalises immediately after FMD.
Method
The study included CMI patients undergoing FMD with perioperative ICP monitoring as a part of clinical management. The pulsatile and static ICP scores were retrieved from the department’s ICP database, and the clinical and radiological data from the patient records.
Results
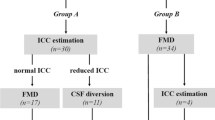
Eleven patients were included in the study. During the first 3 days following FMD, mixed model analysis revealed no significant time-dependent differences of preoperatively elevated either pulsatile (mean wave amplitude, MWA; p = 0.85) and/or static (mean ICP, p = 0.90) ICP. Percentage of mean ICP >15 mmHg increased during days 2 and 3 after FMD. Two patients from the present series had to receive ventriculoperitoneal shunt after FMD in the early postoperative period.
Conclusions
The present observations suggest that anatomical restoration of cerebrospinal fluid pathways by FMD does not lead to immediate normalisation of preoperatively altered pulsatile and static ICP in patients with CMI. This finding may explain persistent symptoms during the early period after FMD.


Similar content being viewed by others


References
Bahl A, Murphy M, Thomas N, Gullan R (2011) Management of infratentorial subdural hygroma complicating foramen magnum decompression: a report of three cases. Acta Neurochir (Wien) 153:1123–1128
Batzdorf U, McArthur DL, Bentson JR (2013) Surgical treatment of Chiari malformation with and without syringomyelia: experience with 177 adult patients. J Neurosurg 118:232–242
Chiari H (1987) Concerning alterations in the cerebellum resulting from cerebral hydrocephalus. Pediatr Neurosci 13:3–8
Eide PK, Kerty E (2011) Static and pulsatile intracranial pressure in idiopathic intracranial hypertension. Clin Neurol Neurosurg 113:123–128
Eide PK, Sorteberg W (2007) Association among intracranial compliance, intracranial pulse pressure amplitude and intracranial pressure in patients with intracranial bleeds. Neurol Res 29:798–802
Eide PK, Sorteberg W (2010) Diagnostic intracranial pressure monitoring and surgical management in idiopathic normal pressure hydrocephalus: a 6-year review of 214 patients. Neurosurgery 66:80–91
Elton STR, Wellons JC, Blounta JP, Grabb PA, Oakes WJ (2002) Acute hydrocephalus following a Chiari I decompression. Pediatr Neurosurg 36:101–104
Filis AK, Moon K, Cohen AR (2009) Symptomatic subdural hygroma and hydrocephalus following Chiari I decompression. Pediatr Neurosurg 45:425–428
Frič R, Eide PK (2015) Comparison of pulsatile and static pressures within the intracranial and lumbar compartments in patients with Chiari malformation type 1: a prospective observational study. Acta Neurochir (Wien) 157:1411–1423
Hayhurst C, Osman-Farah J, Das K, Mallucci C (2008) Initial management of hydrocephalus associated with Chiari malformation type I-syringomyelia complex via endoscopic third ventriculostomy: an outcome analysis. J Neurosurg 108:1211–1214
Klekamp J (2012) Surgical treatment of Chiari I malformation—analysis of intraoperative findings, complications, and outcome for 371 foramen magnum decompressions. Neurosurgery 71:365–380, discussion 380
Marshman LA, Benjamin JC, Chawda SJ, David KM (2005) Acute obstructive hydrocephalus associated with infratentorial subdural hygromas complicating Chiari malformation Type I decompression. Report of two cases and literature review. J Neurosurg 103:752–755
Milhorat TH, Chou MW, Trinidad EM, Kula RW, Mandell M, Wolpert C, Speer MC (1999) Chiari I malformation redefined: clinical and radiographic findings for 364 symptomatic patients. Neurosurgery 44:1005–1017
Perrini P, Rawlinson A, Cowie RA, King AT (2008) Acute external hydrocephalus complicating craniocervical decompression for syringomyelia-Chiari I complex: case report and review of the literature. Neurosurg Rev 31:331–335
Poca MA, Sahuquillo J, Ibanez J, Amoros S, Arikan F, Rubio E (2002) Intracranial hypertension after surgery in patients with Chiari I malformation and normal or moderate increase in ventricular size. Acta Neurochir (Wien) Suppl 81:35–38
Ranjan ACI (1996) Symptomatic subdural hygroma as a complication of foramen magnum decompression for hindbrain herniation (Arnold-Chiari deformity). Br J Neurosurg 10(3):301–303
Tisell M, Wallskog J, Linde M (2009) Long-term outcome after surgery for Chiari I malformation. Acta Neurol Scand 120:295–299
Williams B (1980) Cough headache due to craniospinal pressure dissociation. Arch Neurol 37:226–230
Zakaria R, Kandasamy J, Khan Y, Jenkinson MD, Hall SR, Brodbelt A, Pigott T, Mallucci CL (2012) Raised intracranial pressure and hydrocephalus following hindbrain decompression for Chiari I malformation: a case series and review of the literature. Br J Neurosurg 26:476–481
Acknowledgments
The authors thank Are Hugo Pripp, PhD, Department of Biostatistics, Epidemiology and Health Economics, Oslo University Hospital, Oslo, for performing the statistical mixed model analysis. We thank also Matthew Spreadbury for kindly reviewing the text of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for this research.
Conflict of interest
The first author (R.F.) certifies that he has no affiliations with or involvement in any organisation or entity with any financial interest (such as honoraria, educational grants, participation in speakers’ bureaus, membership, employment, consultancies, stock ownership, or other equity interest, and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript. The software used for analysis of the ICP recordings (Sensometrics Software) is manufactured by a software company (dPCom AS, Oslo, Norway), in which the second author (P.K.E.) has a financial interest.
Ethical approval
For this type of (retrospective) study formal consent is not required. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Comments
In this small and well-written study the authors analyse the ICP pressure pattern (pulsatile and static) in patients with Chiari I malformation, treated with foramen magnum decompression (FMD). The main finding of the study is a delay normalisation of the ICP in those patients with abnormal pre-operative ICP. Chiari I malformation is a different pathophysiological entity from Chiari II. Alteration of the CSF dynamic can be the primary cause of the Chiari I malformation with tonsillar herniation (and other symptoms) as epiphenomena. Identification of those patients with primary raised CSF pressure is of primary importance because a simple CSF diversion procedure can be sufficient [1]. On the other hand, the findings of the authors with delay normalisation of the ICP waveform indicate the necessity to closely monitor post-decompression patients to minimise CSF-related post-operative complication. Should we routinely ICP monitor patients with Chiari malformation following FMD? Should we consider pre-operative ICP monitoring in patient with Chiari I? Possibly the answer is yes, but a larger cohort of patients will be necessary before reaching a final conclusion. The authors should be complimented for the low rate of complication reported as well.
Jibril Osman Farah
Liverpool, UK
1. Hayhurst C, Osman-Farah J, Das K, Mallucci C (2008) Initial management of hydrocephalus associated with Chiari malformation Type I-syringomyelia complex via endoscopic third ventriculostomy: an outcome analysis. J Neurosurg 108:1211–1214
This is a rather preliminary paper on perioperative monitoring of pulsatile and static ICP parameters in patients with Chiari malformation in which the authors investigated the hypothesis that respective values normalise immediately after FMD for patients with CMI 1, and this is the first study also describing changes in pulsatile ICP. ICP waveform monitoring via an intraparenchymal monitor was performed for all patients. A specific automated software algorithm was used for analysis. ICP scores were retrieved from the department’s ICP database. Clinical outcome was reassessed after a mean follow-up of 12 months. The authors’ observations suggest that anatomical restoration of CSF pathways by FMD does not lead to immediate normalisation of preoperatively altered pulsatile and static ICP in patients with CMI. This finding may explain persistent symptoms after FMD. This observation is surprising and deserves further investigation—especially when made in combination with comprehensive imaging studies utilising modern radiographic CSF flow techniques.
Ekkehard Matthias Kasper
Boston, USA
Rights and permissions
About this article

Cite this article
Frič, R., Eide, P.K. Perioperative monitoring of pulsatile and static intracranial pressure in patients with Chiari malformation type 1 undergoing foramen magnum decompression. Acta Neurochir 158, 341–347 (2016). https://doi.org/10.1007/s00701-015-2669-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-015-2669-0