
Abstract
Background
In this pilot study we compared advantages and drawbacks of near-infrared indocyanine green videoangiography (ICGVA) and intraoperative computed tomography (iCT) to investigate if these are complementary or competitive methods to acquire immediate information about blood vessels and potential critical impairment of brain perfusion during vascular neurosurgery.
Methods
A small subset of patients (n = 10) were prospectively enrolled in this feasibility study and received ICGVA immediately after placement of the aneurysm clips. An intraoperative cranial CT angiography (iCTA) was followed by dynamic perfusion CT scan (iCTP) using a 40-slice, sliding-gantry, CT scanner. The vascular patency of major (aneurysm bearing) arteries, visualisation of arising perforating arteries and brain perfusion after clip application were analysed with both techniques.
Results
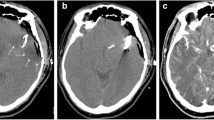
The ICGVA was able to visualise blood flow and vascular patency of all major vessels and perforating arteries within the visual field of the microscope, but failed to display vessels located within deeper areas of the surgical field. Even small coverage with brain parenchyma impaired detection of vessels. With iCTA high image quality could be obtained in 7/10 cases of clipped aneurysms. Intraoperative CTA was not sufficiently evaluable in one PICA aneurysm and one case of a previously coiled recurrent aneurysm, due to extensive coil artefacts. Small, perforating arteries could not be detected with iCTA. Intraoperative CTP allowed the assessment of global blood flow and brain perfusion in sufficient quality in 5/10 cases, and enabled adequate intraoperative decision making.
Conclusion
A combination of ICGVA and iCT is feasible, with very good diagnostic imaging quality associated with short acquisition time and little interference with the surgical workflow. Both techniques are complementary rather than competing analysing tools and help to assess information about local (ICGVA/iCTA) as well as regional (iCTA/iCTP) blood flow and cerebral perfusion immediately after clipping of intracranial aneurysms.



Similar content being viewed by others


References
Alexander TD, Macdonald RL, Weir B, Kowalczuk A (1996) Intraoperative angiography in cerebral aneurysm surgery: a prospective study of 100 craniotomies. Neurosurgery 39(1):10–17
Chiang VL, Gailloud P, Murphy KJ, Rigamonti D, Tamargo RJ (2002) Routine intraoperative angiography during aneurysm surgery. J Neurosurg 96(6):988–992
Dashti R, Laakso A, Niemela M, Porras M, Hernesniemi J (2009) Microscope-integrated near-infrared indocyanine green videoangiography during surgery of intracranial aneurysms: the Helsinki experience. Surg Neurol 71(5):543–550
Dehdashti AR, Thines L, Da Costa LB, terBrugge KG, Willinsky RA, Wallace MC, Tymianski M (2009) Intraoperative biplanar rotational angiography during neurovascular surgery. Technical note. J Neurosurg 111(1):188–192
de Oliveira JG, Beck J, Seifert V, Teixeira MJ, Raabe A (2008) Assessment of flow in perforating arteries during intracranial aneurysm surgery using intraoperative near-infrared indocyanine green videoangiography. Neurosurgery 62(6 Suppl 3):1300–1310
Doenitz C, Schebesch KM, Zoephel R, Brawanski A (2010) A mechanism for the rapid development of intracranial aneurysms: a case study. Neurosurgery 67(5):1213–1221
Faber F, Thon N, Fesl G, Rachinger W, Guckler R, Tonn JC, Schichor C (2011) Enhanced analysis of intracerebral arterioveneous malformations by the intraoperative use of analytical indocyanine green videoangiography: technical note. Acta Neurochir (Wien) 153(11):2181–2187
Friedman JA, Kumar R (2009) Intraoperative angiography should be standard in cerebral aneurysm surgery. BMC Surg 9:7
Klopfenstein JD, Spetzler RF, Kim LJ, Feiz-Erfan I, Han PP, Zabramski JM, Porter RW, Albuquerque FC, McDougall CG, Fiorella DJ (2004) Comparison of routine and selective use of intraoperative angiography during aneurysm surgery: a prospective assessment. J Neurosurg 100(2):230–235
Molyneux AJ (2005) Indications for treatment of cerebral aneurysms from an endovascular perspective: the creation of an evidence base for interventional techniques. Neurosurg Clin N Am 16(2):313–316, ix
Molyneux AJ, Kerr RS (2002) The future management of subarachnoid haemorrhage. J Neuroradiol 29(2):74–75
Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, Sandercock P (2005) International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 366(9488):809–817
Pechlivanis I, Konig M, Engelhardt M, Scholz M, Heuser L, Harders A, Schmieder K (2009) Evaluation of clip artefacts in three-dimensional computed tomography. Cen Eur Neurosurg 70(1):9–14
Raabe A, Beck J, Gerlach R, Zimmermann M, Seifert V (2003) Near-infrared indocyanine green video angiography: a new method for intraoperative assessment of vascular flow. Neurosurgery 52(1):132–139
Raabe A, Beck J, Seifert V (2005) Technique and image quality of intraoperative indocyanine green angiography during aneurysm surgery using surgical microscope integrated near-infrared video technology. Zentralbl Neurochir 66(1):1–6
Raftopoulos C, Vaz G (2011) Surgical indications and techniques for failed coiled aneurysms. Adv Tech Stand Neurosurg 36:199–226
Schichor C, Rachinger W, Morhard D, Zausinger S, Heigl TJ, Reiser M, Tonn JC (2010) Intraoperative computed tomography angiography with computed tomography perfusion imaging in vascular neurosurgery: feasibility of a new concept. J Neurosurg 112(4):722–728
Tonn JC, Schichor C, Schnell O, Zausinger S, Uhl E, Morhard D, Reiser M (2011) Intraoperative computed tomography. Acta Neurochir Suppl 109:163–167
Wachter D, Psychogios M, Knauth M, Rohde V (2010) IvACT after aneurysm clipping as an alternative to digital subtraction angiography—first experiences. Cen Eur Neurosurg 71(3):121–125
Zachenhofer I, Cejna M, Schuster A, Donat M, Roessler K (2010) Image quality and artefact generation post-cerebral aneurysm clipping using a 64-row multislice computer tomography angiography (MSCTA) technology: a retrospective study and review of the literature. Clin Neurol Neurosurg 112(5):386–391
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
The comparison of the described techniques is of scientific interest and iCTA may definitely be helpful for the vascular neurosurgeon in some special situations in addition to or instead of the other techniques with their limitations. The problem may be that we do not know without intraoperative—and also somewhat time-consuming—conventional angiography which of the techniques (ICGVA or iCTA) is to be trusted during surgery. With usually limited resources, the purchase of the relatively slow and complex technique of iCTA would further increase the indirect expenses of clipping in addition to already having the expensive microscopes equipped with ICGVA. Naturally, patient safety comes first, but it is doubtful whether iCTA is a necessity in everyday practice, even in a dedicated neurovascular centres.
Mika Niemelä
Juha Hernesniemi
Helsinki, Finland
Rights and permissions
About this article
Cite this article
Schnell, O., Morhard, D., Holtmannspötter, M. et al. Near-infrared indocyanine green videoangiography (ICGVA) and intraoperative computed tomography (iCT): are they complementary or competitive imaging techniques in aneurysm surgery?. Acta Neurochir 154, 1861–1868 (2012). https://doi.org/10.1007/s00701-012-1386-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-012-1386-1