
Abstract
Purpose
Preoperative pulmonary dysfunction has been associated with increased operative mortality and morbidity after cardiac surgery. This study aimed to determine whether values for the diffusing capacity of the lung for carbon monoxide (DLCO) could predict postoperative complications after cardiac surgery.
Methods
This study included 408 consecutive patients who underwent cardiac surgery between June 2008 and December 2015. DLCO was routinely determined in all patients. A reduced DLCO was clinically defined as %DLCO < 70%. %DLCO was calculated as DLCO divided by the predicted DLCO. The association between %DLCO and in-hospital mortality was assessed, and independent predictors of complications were identified by a logistic regression analysis.
Results
Among the 408 patients, 338 and 70 had %DLCO values of ≥ 70% and < 70%, respectively. Complications were associated with in-hospital mortality (P < 0.001), but not %DLCO (P = 0.275). A multivariate logistic regression analysis with propensity score matching identified reduced DLCO as an independent predictor of complications (OR, 3.270; 95%CI, 1.356–7.882; P = 0.008).
Conclusions
%DLCO is a powerful predictor of postoperative complications. The preoperative DLCO values might provide information that can be used to accurately predict the prognosis after cardiac surgery.
Clinical trial registration number
UMIN000029985.
Similar content being viewed by others

Introduction
Preoperative pulmonary dysfunction in chronic obstructive pulmonary disease (COPD) has been considered to be associated with increased operative mortality and morbidity after cardiac surgery. A careful evaluation of the pulmonary function before and after cardiac surgery demonstrated a significant reduction in lung volume, diffusion capacity, and oxygenation at 2 weeks after surgery, with partial improvement after 4 months [1]. The preoperative identification of patients who are at greater risk of developing complications is important to prevent postoperative complications and obtain a good operative outcome.
The analysis of the diffusing capacity of the lung for carbon monoxide (DLCO) is a clinically useful pulmonary function test (PFT). Unlike other spirometric measurements, DLCO is less influenced by patient effort [2]. DLCO represents the ability of the lung to diffuse carbon monoxide across its membranes and assesses the transfer of gases from the alveoli to red blood cells. The diffusion of O2 depends on the following factors: the alveolar ventilation/capillary perfusion ratio, which establishes the partial pressure gradient of O2 between the alveoli and plasma; the physical characteristics of the alveolar–capillary interface; the capillary blood volume available for gas exchange; the hemoglobin (Hb) concentration; and the reaction rate between O2 and Hb [3, 4]. The diffusion characteristics of the lung are commonly assessed by tests of CO transfer. CO diffuses across the alveoli and binds to Hb with 240-fold greater affinity than O2 [3]. DLCO depends on two resistances arranged in series according to the following equation:
1/DLCO = 1/DM + 1/θCOVC [3,4,5], where DM is the alveolar–capillary membrane conductance, θCO is the rate of CO uptake by the whole blood combined with Hb measured in vitro, and VC is the lung capillary blood volume [3,4,5]. A decline in DLCO can occur as a result of destruction of alveolar structures, distal airway dysfunction, contraction of the pulmonary capillary volume due to ventilation, perfusion abnormalities, and Hb abnormalities.
DLCO is an equally powerful predictor of postoperative complications in patients with and without COPD after lung resection. A previous study suggested that DLCO should be routinely measured during preoperative evaluations, regardless of whether a patient’s spirometric values are abnormal [2].
Another study reported that reduced alveolar–capillary membrane conductance is associated with pulmonary congestion [6]. Thus, DLCO may be influenced by pulmonary edema and fluid accumulation in the interstitial spaces before and after cardiac surgery. The present study aimed to determine whether DLCO can serve as a predictor of complications arising after cardiac surgery.
Patients and methods
Patients
The study protocol was approved by the Institutional Review Board of the Dokkyo Medical University. Between June 2008 and December 2015, 2040 patients underwent cardiac surgery at Dokkyo Medical University Hospital. A total of 408 patients in whom preoperative DLCO values were routinely collected within 1 week before scheduled cardiac surgery were included in this study. The attending physician for each patient made the decision to proceed with the PFT, which included measurement of DLCO, based on clinical indications. The exclusion criteria were any emergency or urgent operation, aortic surgery, beating heart surgery, and approaches other than median sternotomy. We reviewed the medical records of the patients, including the demographics, preoperative clinical data, PFT findings, hemodynamic data from cardiac catheterization, and operative and postoperative data.
DLCO measurement and %DLCO
We measured DLCO in a single-breath-hold maneuver with the patient seated upright in a chair with their nostrils closed with a clip. The patients then breathed normally and exhaled to residual volume, and then, a carbon monoxide–helium mixture was forcefully inhaled to total lung capacity, and held for 10 s and then exhaled. The patients exhaled to wash out the estimated mechanical and anatomical dead space. Alveolar samples were then collected, and DLCO was calculated from the total volume of the lung, breath-hold duration, and the initial and final alveolar concentrations of CO. The exhaled helium concentration was used to determine a single-breath estimate of the total lung capacity and the initial alveolar concentration of CO. The predicted DLCO was determined from regression equations according to age, height, and sex (predicted DLCO for men, 15.5 × body surface area (BSA) − 0.23 × age + 6.8; predicted DLCO for women, 15.5 × BSA − 0.117 × age + 0.5) [7]. %DLCO was calculated by dividing the actual DLCO by the predicted DLCO.
Surgical technique
A median sternotomy approach was applied under general anesthesia to all patients. Cardiopulmonary bypass (CPB) was established through the ascending aorta or by right atrial or bicaval cannulation. The myocardium was protected by antegrade and retrograde cardioplegia with intermittent cold-blood cardioplegia and reperfusion with warm-blood cardioplegia. A normothermic temperature was maintained during CPB. The patients were transferred to the intensive care unit immediately after the procedure with ventilator assistance and monitoring.
Definitions of complications
Postoperative outcomes were defined according to the Society of Thoracic Surgeons National Database as follows. In-hospital death was defined as the death of a patient due to any cause during hospitalization in the institution, where they underwent cardiac surgery. Stroke was defined as a central neurologic deficit persisting for > 72 h. Wound infection was defined as infection involving subcutaneous tissue, muscle, bone, or the mediastinum, and requiring surgical intervention. Respiratory complications were also included. The incidence of postoperative respiratory complications was scored on an ordinal scale of 1–4, using the operational definitions of postoperative pulmonary complications described by Kroenke et al. [8] (Table 1) . Clinically significant respiratory complications were defined as one item among grade 3 or 4 complications.
Statistical analysis
Continuous variables are expressed as the mean ± standard deviation (SD) and were compared using Student’s t test or the Mann–Whitney test, as appropriate. Nominal variables are expressed as percentages and were analyzed using the χ2 test or Fisher’s exact probability test. All variables with P values of < 0.20 in the univariate analysis were included in the multivariable analyses. Other clinically relevant variables, namely, sex, age, body mass index (BMI), and BSA, were adjusted in the multivariable analysis. Independent predictors of postoperative complications after cardiac surgery were identified using a multivariate logistic regression model with the forced entry method. Odds ratios (OR), 95% confidence intervals (95%CI), and P values are reported. To minimize selection bias derived from the retrospective observational study design, propensity score analyses were performed to generate two groups, considering the following covariates: age, sex, BMI, %VC, and hemoglobin. 70 patients with %DLCO < 70% and 67 patients with %DLCO ≥ 70% were matched. A logistic regression analysis for the abovementioned covariates, with nearest-neighbor one-to-one matching, was performed to determine the propensity scores. All statistical tests were two-sided, and P values of < 0.05 were considered to indicate statistical significance. All statistical analyses were performed using the IBM SPSS statistics 24 software program (IBM, Armonk, NY, USA).
Results
Patient characteristics and outcomes
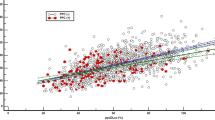
Table 2 summarizes the characteristics of the 408 patients (age, 66.0 ± 10.0 years; male, n = 295 [72.3%]), whose data were analyzed in this study. Isolated coronary artery bypass grafting (CABG) was performed for 224 (54.9%) patients, and 184 (45.9%) underwent valve surgery (including concomitant cardiac surgery). Six (1.47%) patients died in hospital due to multi-organ failure (n = 1), sudden death (n = 1), and sepsis (n = 4). Operative complications developed in 91 (22.3%) patients and consisted of gastrointestinal disorder (n = 3), stroke (n = 4), renal disorder (n = 5), cardiac disorder (n = 7), wound infection (n = 19), and respiratory complications (n = 71; Grade 3: n = 61, Grade 4: n = 3). Figures 1 and 2 show the relationship between patients with all complications or respiratory complications and %DLCO by quartile. The incidence of all complications significantly differed in Q1 (OR, 3.323; 95%CI, 1.472–7.500; P = 0.005); the OR for respiratory complications was 3.462 (95%CI, 1.434–8.357; P = 0.005). Although a DLco value of < 80% of the predicted value was considered abnormal, according to a previous definition by Steenhuis et al. [9], the incidence of complications differed in Q1 (%DLco < 74.6%). A DLco value of < 70% the predicted value was considered to be the cut-off value. The area under the receiver operating characteristic curve values was 0.625 (95%CI 0.558–0.692) for all complications and 0.632 (95%CI 0.557–0.707) for respiratory complications. The sensitivity and specificity of %DLco, with a cut-off value of 70%, were 0.864 and 0.297, respectively, for all complications (0.861 and 0.324 for respiratory complications).

Patients with all complications after surgery and the %DLCO quartiles. The %DLCO quartiles were as follows: Q1 (≤ 74.6%), Q2 (74.7–88.8%), Q3 (88.9–101.7%), and Q4 (≥ 101.8%). DLCO diffusing capacity of lung for carbon monoxide, OR odds ratio. Error bars represent 95% confidence intervals. OR adjusted for sex, age, body mass index, body surface area, hemoglobin A1C, New York Heart Association class, atrial fibrillation, brain natriuretic peptide, %vital capacity, hemoglobin, logistic Euro score II, STS score, durations of surgery, pump, and aortic clamp

Patients with respiratory complications after surgery and the %DLCO quartiles. The %DLCO quartiles were as follows: Q1 (≤ 74.6%), Q2 (74.7–88.8%), Q3 (88.9–101.7%), and Q4 (≥ 101.8%). The ORs were adjusted as described in the Fig. 1 legend. DLCO diffusing capacity of lung for carbon monoxide, OR odds ratio. Error bars represent 95% confidence intervals
Preoperative demographics and clinical variables according to the %DLCO risk
Table 2 shows the preoperative and perioperative factors of patients with %DLCO of ≥ 70% (n = 338) or < 70% (n = 70). Significant differences were observed in age (66.5 ± 9.70 vs. 63.8 ± 11.2 years; P = 0.036) and sex (female) (86 [25.4%] vs. 27 [38.6%]; P = 0.025). There were no significant differences in the risk factors, which included hypertension, hyperlipidemia, history of smoking, BMI, BSA, and HbA1C. Among the clinical and biochemical parameters, significant differences were observed in extracardiac arteriopathy (52 [15.4%] vs. 21 [30.0%]; P = 0.004) and Hb (13.1 ± 1.7 vs. 12.3 ± 1.9 g/dL; P < 0.001). In terms of the cardiac function, the brain natriuretic peptide (BNP) levels of the two groups were significantly different (193.6 ± 381.3 vs. 265.3 ± 497.1 pg/mL; P = 0.023), whereas ejection fraction was not (57.7% ± 13.7% vs. 56.0% ± 14.0%; P = 0.345). Among the factors associated with the respiratory function, %VC was significantly different (95.65 ± 16.1% vs. 89.6 ± 16.5%; P = 0.005), whereas FEV1.0% was not (72.6 ± 10.1% vs. 72.4 ± 12.6%; P = 0.878). Among the factors associated with the renal function, the serum creatinine level did not differ to a statistically significant extent (1.3 ± 1.7 vs. 1.3 ± 1.7 mg/dL; P = 0.306).
CABG was the only operative method for which there was significant difference (193 [57.1%] vs. 31 [44.3%] P = 0.050). The operative time (322.5 ± 79.2 vs. 323 ± 85.3 min; P = 0.350), pump time (144.3 ± 49.9 vs. 152.0 ± 51.5 min; P = 0.244), and aortic clamp time (105.0 ± 22.6 vs. 110.2 ± 40.5 min; P = 0.347) did not differ to a statistically significant extent. Furthermore, there was no significant difference in the rate of hospital mortality (4 [1.2%]) vs. 2 [2.9%]; P = 0.275. There were significant differences between the two groups in the rates of all complications (64 [18.9%] vs. 27 [38.6%]; P < 0.001) and respiratory complications (48 [14.2%] vs. 23 [32.9%]; P < 0.001).
%DLCO as a predictor of complications after cardiac surgery
Table 3 shows the results of the univariate analysis of patients with all complications and those with respiratory complications. Among the preoperative data, significant differences were observed in the rates of %DLCO < 70%, BNP ≥ 100 pg/mL, Hb < 11 g/dL, and the Euro Score II and STS score values of the patients with and without all and those with and without respiratory complications. Among the perioperative factors, significant differences were observed in the operative time, the pump time and the aortic clamp time between the patients with and without complications. A multivariate logistic regression analysis identified BMI (OR, 1.156; 95%CI, 1.039–1.286; P = 0.008), BSA (OR, 0.040; 95%CI, 0.003–0.575; P = 0.018), and a reduced %DLCO (OR, 2.682; 95%CI, 1.449–4.962; P = 0.002) as preoperative factors that were significant independent predictors of all complications. Pump time (OR, 1.016; 95%CI, 1.003–1.030; P = 0.017) as identified as a perioperative factor that was a significant predictor of all complications (Table 4). The multivariate logistic regression analysis identified a reduced %DLCO (OR, 2.833; 95%CI, 1.490–5.398; P = 0.001) and increased HbA1C (OR, 2.284; 95%CI. 1.102–4.733; P = 0.026) as preoperative factors that were significant independent predictors of respiratory complications (Table 5). The propensity score analysis identified a reduced %DLCO as a predictor of all complications and respiratory complications: all complications (OR, 3.270; 95%CI, 1.356–7.882; P = 0.008) and respiratory complications (OR, 3.447; 95%CI, 1.343–8.846; P = 0.010) (Table 6).
Discussion
The principal finding of this study was that the preoperative DLCO was correlated with postoperative complications after cardiac surgery. Others have described significant and prolonged impairment of the pulmonary function after cardiac surgery [1]. Decreased ventilation, pulmonary disease, and reduced alveolar perfusion caused by poor cardiac output and chronic heart failure might also influence DLCO [10]. DLCO is a clinically useful indicator of the lung function, because it assesses gas transfer from the alveoli to the red blood cells. The preoperative DLCO is not routinely measured in patients in most cardiac surgery units. Reduced postoperative capillary filtration due to basal membrane thickening, enhanced alveolar fluid clearance, and increased lymphatic drainage leads to restricted lung spirometry and impaired gas transfer [6]. We hypothesized that the postoperative DLCO might be more decreased than the preoperative DLCO and that this could serve as a predictor of early complications after cardiac surgery. The present study found that more postoperative complications developed among patients with %DLCO of < 70% than among those with %DLCO of > 70%. A previous study also found that patients with stable chronic heart failure had decreased %VC values, in addition to decreased DLCO and DM values [11]. The present study showed that the %VC values were decreased and the BNP levels were increased in patients with lower DLCO values; however, these patients might have had preoperative chronic heart failure. Thus, %DLCO might be a marker of heart failure.
A previous study suggested that cardiac surgery may also contribute to a greater reduction in DLCO. The mechanism underlying the reduction of DLCO after cardiac surgery is unclear. One hypothesis is that it might reflect pathophysiological changes in the pulmonary microcirculation initiated by CPB, such as a systemic inflammatory response with coagulopathy and altered microvascular permeability [12]. That CPB interferes with pulmonary function has been established. It can induce adverse effects on alveolar stability by activating the complement cascade, sequestering neutrophils in the pulmonary microvascular bed, releasing oxygen-derived free radicals, and changing the composition of alveolar surfactant [13]. The mechanism underlying the diffusion impairment after cardiac surgery could be caused by pulmonary edema and the accumulation of fluid in interstitial spaces, ventilation–perfusion mismatches, or changes in Hb concentrations [14]. A few studies have identified a relationship between DLCO and the outcomes after cardiac surgery. Published data show that a %DLCO value of < 50% the predicted value at the preoperative PFT is an independent risk factor for a > threefold increase in mortality after adjustment for mortality risk estimates [15]. Few patients in the present study had a %DLCO value of < 50%. Thus, our analysis included %DLCO < 70% as an approximation for Q1. The findings of the present study showed that %DLCO < 70% in a preoperative PFT was independently associated with a > 3.3-fold increase in risk for all complications after adjustment for morbidity risk estimates; the risk of respiratory complications was increased > 3.4-fold.
Postoperative respiratory complications continue to affect patient morbidity and mortality, length of hospital stay, and overall resource utilization, despite advances in preoperative, intraoperative. and postoperative care [16,17,18]. Respiratory muscle dysfunction due to surgery can lead to a reduced vital capacity, tidal volume, and total lung capacity [19]. This could cause atelectasis in the basal lung segments and decrease the functional residual capacity, which affects pulmonary gas exchange properties by increasing ventilation/perfusion mismatches. Thus, DLCO might also decrease after surgery. Preoperative and postoperative chest physical therapy has significantly reduced the number of patients who develop atelectasis, but it does not significantly benefit patients who develop respiratory complications due to infection [20]. Improving the preoperative respiratory status of these patients via the fine adjustment of medication therapy and strict physiotherapeutic control seems important. Preoperative short-term pulmonary rehabilitation for such patients improves the pulmonary function and reduces the incidence of atelectasis, consolidation, and pneumothorax [16]. Preoperative physical therapy with inspiratory muscle training for at least 2 weeks reduced the incidence of postoperative pulmonary complications by 50% [18]. Although the present study did not uncover evidence as to whether surgical outcomes would improve with preoperative short-term pulmonary rehabilitation, determining the correct timing of surgery is also important for avoiding respiratory decompensation.
The present study is associated with several limitations. Although all data were prospectively recorded, this was a retrospective, single-institute study. The retrospective design is susceptible to various sources of bias, which might have not been identified or controlled. The preoperative PFTs were performed according to requests from clinicians, who were not blinded to the results of the PFT. Thus, the possibility that patient management might have been affected by the PFT results cannot be excluded.
In conclusion, the %DLCO seems to be a powerful predictor of postoperative complications. To the best of our knowledge, this is one of the few studies to assess whether DLCO is a potential risk factor for adverse outcomes of patients after cardiac surgery. Preoperative DLCO values might provide more accurate prognostic information about outcomes after cardiac surgery. Preoperative PFT findings might provide clinicians with more accurate risk profiles as well as additional prognostic information. Thus, pulmonary function testing, including measurement of DLCO, should be a routine component of preoperative evaluations.
References
Braun SR, Birnbaum ML, Chopra PS. Pre- and postoperative pulmonary function abnormalities in coronary artery revascularization surgery. Chest. 1978;73:316–20.
Ferguson MK, Lehman AG, Bolliger CT, Brunelli A. The role of diffusing capacity and exercise tests. Thorac Surg Clin. 2008;18:9–17.
Guazzi M. Alveolar-capillary membrane dysfunction in heart failure: evidence of a pathophysiologic role. Chest. 2003;124:1090–102.
Guazzi M. Alveolar-capillary membrane dysfunction in chronic heart failure: pathophysiology and therapeutic implications. Clin Sci. 2000;98:633–41.
Guazzi M. Alveolar gas diffusion abnormalities in heart failure. J Cardiac Fail. 2008;14:695–702.
Melenovsky V, Andersen MJ, Andress K, Reddy YN, Borlaug BA. Lung congestion in chronic heart failure: haemodynamic, clinical, and prognostic implications. Eur J Heart Fail. 2015;17:1161–71.
Burrows B, Kasik JE, Niden AH, Barclay WR. Clinical usefulness of the single-breath pulmonary diffusing capacity test. Am Rev Respir Dis. 1961;84:789–806.
Kroenke K, Lawrence VA, Theroux JF, Tuley MR. Operative risk in patients with severe obstructive pulmonary disease. Arch Intern Med. 1992;152:967–71.
Steenhuis LH, Groen HJ, Koëter GH, van der Mark TW. Diffusion capacity and haemodynamics in primary and chronic thromboembolic pulmonary hypertension. Eur Respir J. 2000;16(2):276–81.
Shapira N, Zabatino SM, Ahmed S, Murphy DM, Sullivan D, Lemole GM. Determinants of pulmonary function in patients undergoing coronary bypass operations. Ann Thorac Surg. 1990;50:268–73.
Agostoni P, Bussotti M, Cattadori G, Margutti E, Contini M, Muratori M, et al. Gas diffusion and alveolar–capillary unit in chronic heart failure. Eur Heart J. 2006;27:2538–43.
Johnson BD, Beck KC, Olson LJ, O’Malley KA, Allison TG, Squires RW, et al. Pulmonary function in patients with reduced left ventricular function: influence of smoking and cardiac surgery. Chest. 2001;120:1869–76.
Güler M, Kirali K, Toker ME, Bozbuğa N, Omeroğlu SN, Akinci E, et al. Different CABG methods in patients with chronic obstructive pulmonary disease. Ann Thorac Surg. 2001;71:152–7.
Westerdahl E, Lindmark B, Bryngelsson I, Tenling A. Pulmonary function 4 months after coronary artery bypass graft surgery. Respir Med. 2003;97:317–22.
Adabag AS, Wassif HS, Rice K, Mithan S, Johnson D, Bonawitz-Conlin J, et al. Preoperative pulmonary function and mortality after cardiac surgery. Am Heart J. 2010;159:691–7.
Scott BH, Seifert FC, Grimson R, Glass PS. Octogenarians undergoing coronary artery bypass graft surgery: resource utilization, postoperative mortality, and morbidity. J Cardiothorac Vasc Anesth. 2005;19:583–8.
Toumpoulis IK, Anagnostopoulos CE, Balaram SK, Rokkas CK, Swistel DG, Ashton RC Jr, et al. Assessment of independent predictors for long-term mortality between women and men after coronary artery bypass grafting: are women different from men? J Thorac Cardiovasc Surg. 2006;131:343–51.
Hulzebos EH, Helders PJ, Favié NJ, De Bie RA, Brutel de la Riviere A, Van Meeteren NL. Preoperative intensive inspiratory muscle training to prevent postoperative pulmonary complications in high-risk patients undergoing CABG surgery: a randomized clinical trial. JAMA. 2006;296:1851–7.
Wynne R, Botti M. Postoperative pulmonary dysfunction in adults after cardiac surgery with cardiopulmonary bypass: clinical significance and implications for practice. Am J Crit Care. 2004;13:384–93.
Castillo R, Haas A. Chest physical therapy: comparative efficacy of preoperative and postoperative in the elderly. Arch Phys Med Rehabil. 1985;66:376–9.
Acknowledgements
The authors thank Yasuo Haruyama, MD, PhD, Department of Public Health, Dokkyo Medical University, for helping with the statistical analyses.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest in association with the present study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Kuwata, T., Shibasaki, I., Ogata, K. et al. Lung-diffusing capacity for carbon monoxide predicts early complications after cardiac surgery. Surg Today 49, 571–579 (2019). https://doi.org/10.1007/s00595-019-1770-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-019-1770-z