
Abstract
Purpose
The association between intramedullary increased signal intensity (ISI) on T2-weighted magnetic resonance imaging and surgical outcome in cervical spondylotic myelopathy (CSM) remains controversial. The purpose of this study is to assess the impact of quantitative signal change ratio (SCR) on the surgical outcome for CSM.
Methods
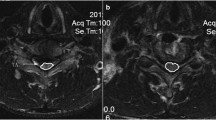
The prospective study included 108 consecutive patients who underwent surgical treatment for CSM. The Japanese Orthopaedic Association (JOA) score and recovery rate were used to evaluate clinical outcomes. JOA recovery rate less than 50 % was defined as a poor clinical result. The SCR was defined as the signal intensity at the level of ISI or severely compressed cord (in cases with no ISI) divided by the signal intensity at the C7–T1 disc level. Age, sex, body mass index, duration of symptoms, surgical technique, preoperative JOA score, levels of compression, preoperative SCR, preoperative C2–7 angle, preoperative C2–7 range of motion were assessed.
Results
Forty patients (37.0 %) had a recovery rate of less than 50 %. Multivariate logistic regression analysis revealed that a higher preoperative SCR and a longer duration of symptoms were significant risk factors for a poor clinical outcome. Receiver operating characteristic (ROC) curve analysis showed that the optimal preoperative SCR cutoff value as a predictor of poor clinical result was 1.46. The area under the ROC curve of preoperative SCR for predicting a poor surgical outcome was 0.844.
Conclusions
Preoperative SCR significantly reflected the surgical outcome in patients with CSM. Patients with SCR greater than or equal to 1.46 can experience poor recovery after surgery.

Similar content being viewed by others


References
Clark CR (1988) Cervical spondylotic myelopathy: history and physical findings. Spine 13:847–849
Clarke E, Robinson PK (1956) Cervical myelopathy: a complication of cervical spondylosis. Brain 79:483–510
Mehalic TF, Pezzuti RT, Applebaum BI (1990) Magnetic resonance imaging and cervical spondylotic myelopathy. Neurosurgery 26:217–226
Okada Y, Ikata T, Yamada H et al (1993) Magnetic resonance imaging study on the results of surgery for cervical compression myelopathy. Spine 18:2024–2029
Matsuda Y, Miyazaki K, Tada K et al (1991) Increased MR signal intensity due to cervical myelopathy. Analysis of 29 surgical cases. J Neurosurg 74:887–892
Suri A, Chabbra RP, Mehta VS et al (2003) Effect of intramedullary signal changes on the surgical outcome of patients with cervical spondylotic myelopathy. Spine J 3:33–45
Takahashi M, Yamashita Y, Sakamoto Y et al (1989) Chronic cervical cord compression: clinical significance of increased signal intensity on MR images. Radiology 173:219–224
Morio Y, Teshima R, Nagashima H et al (2001) Correlation between operative outcomes of cervical compression myelopathy and mri of the spinal cord. Spine 26:1238–1245
Yone K, Sakou T, Yanase M et al (1992) Preoperative and postoperative magnetic resonance image evaluations of the spinal cord in cervical myelopathy. Spine 17:S388–S392
Wada E, Yonenobu K, Suzuki S et al (1999) Can intramedullary signal change on magnetic resonance imaging predict surgical outcome in cervical spondylotic myelopathy? Spine 24:455–461
Alafifi T, Kern R, Fehlings M (2007) Clinical and MRI predictors of outcome after surgical intervention for cervical spondylotic myelopathy. J Neuroimaging 17:315–322
Mastronardi L, Elsawaf A, Roperto R et al (2007) Prognostic relevance of the postoperative evolution of intramedullary spinal cord changes in signal intensity on magnetic resonance imaging after anterior decompression for cervical spondylotic myelopathy. J Neurosurg Spine 7:615–622
Zhang YZ, Shen Y, Wang LF et al (2010) Magnetic resonance T2 image signal intensity ratio and clinical manifestation predict prognosis after surgical intervention for cervical spondylotic myelopathy. Spine 35:E396–E399
Wang LF, Zhang YZ, Shen Y et al (2010) Using the T2-weighted magnetic resonance imaging signal intensity ratio and clinical manifestations to assess the prognosis of patients with cervical ossification of the posterior longitudinal ligament. J Neurosurg Spine 13:319–323
Hirabayashi K, Miyakawa J, Satomi K et al (1981) Operative results and postoperative progression of ossification among patients with ossification of posterior longitudinal ligament. Spine 6:354–364
Furlan JC, Kalsi-Ryan S, Kailaya-Vasan A et al (2011) Functional and clinical outcomes following surgical treatment in patients with cervical spondylotic myelopathy: a prospective study of 81 cases. J Neurosurg Spine 14:348–355
Cheung WY, Arvinte D, Wong YW et al (2008) Neurological recovery after surgical decompression in patients with cervical spondylotic myelopathy—a prospective study. Int Orthop 32:273–278
Tani T, Ushida T, Ishida K et al (2002) Relative safety of anterior microsurgical decompression versus laminoplasty for cervical myelopathy with a massive ossified posterior longitudinal ligament. Spine 27:2491–2498
Uchida K, Nakajima H, Sato R et al (2005) Multivariate analysis of the neurological outcome of surgery for cervical compressive myelopathy. J Orthop Sci 10:564–573
Fujiwara K, Yonenobu K, Ebara S et al (1989) The prognosis of surgery for cervical compression myelopathy. An analysis of the factors involved. J Bone Joint Surg Br 71:393–398
Koyanagi T, Hirabayashi K, Satomi K et al (1993) Predictability of operative results of cervical compression myelopathy based on preoperative computed tomographic myelography. Spine 18:1958–1963
Singh A, Crockard HA, Platts A et al (2001) Clinical and radiological correlates of severity and surgery-related outcome in cervical spondylosis. J Neurosurg 94:189–198
Matsuyama Y, Kawakami N, Mimatsu K (1995) Spinal cord expansion after decompression in cervical myelopathy. Investigation by computed tomography myelography and ultrasonography. Spine 20:1657–1663
Takahashi M, Sakamoto Y, Miyawaki M et al (1987) Increased MR signal intensity secondary to chronic cervical cord compression. Neuroradiology 29:550–556
Al-Mefty O, Harkey LH, Middleton TH et al (1988) Myelopathic cervical spondylotic lesions demonstrated by magnetic resonance imaging. J Neurosurg 68:217–222
Yukawa Y, Kato F, Yoshihara H et al (2007) MR T2 image classification in cervical compression myelopathy: predictor of surgical outcomes. Spine 32:1675–1678
Chen CJ, Lyu RK, Lee ST et al (2001) Intramedullary high signal intensity on T2-weighted MR images in cervical spondylotic myelopathy: prediction of prognosis with type of intensity. Radiology 221:789–794
Okais N, Moussa R, Hage P (1997) Value of increased MRI signal intensity in cervical arthrosis in myelopathies. Neurochirurgie 43:285–290
Acknowledgments
We thank Dr. Jie Li for his assistance in the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest concerning this article.
Additional information
J. T. Zhang and F. T. Meng contributed equally to this work.
J. T. Zhang and F. T. Meng should be considered co-first authors.
Rights and permissions
About this article

Cite this article
Zhang, J.T., Meng, F.T., Wang, S. et al. Predictors of surgical outcome in cervical spondylotic myelopathy: focusing on the quantitative signal intensity. Eur Spine J 24, 2941–2945 (2015). https://doi.org/10.1007/s00586-015-4109-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-4109-5