
Abstract
Background
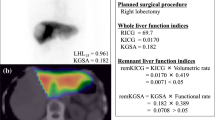
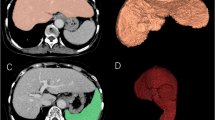
We developed a new combined 99mTc-galactosyl human serum albumin (GSA) scintigraphy single-photon emission computed tomography (SPECT)/CT system to evaluate the changes in functional liver volume with portal vein embolization (PVE).
Methods
We performed a prospective analysis of 25 patients treated with right PVE, and evaluated their functional liver volume perioperatively with a 99mTc-GSA scintigraphy SPECT–CT fusion system. The percentage of the non-tumorous remnant liver volume (%LV) and the percentage of functional remnant liver volume (%FLV) were estimated by using the following calculations: (future remnant volume − tumor volume)/(total liver volume − tumor volume) and functional future remnant liver volume/functional total liver volume, respectively.
Results
Before PVE, the correlation was strongly significant between %LV and %FLV of the non-embolized liver, and the data were nearly equal (the regression coefficient was 1.005, P < 0.0001). In contrast, after PVE, there was a significant correlation between %LV and %FLV (P < 0.0001), but the regression coefficient was 1.192. The % LV increased significantly, from 38.1 to 52.0%, and the increment was 13.9% (P < 0.0005). The %FLV was also increased significantly, from 36.6 to 58.0%, and the increment was 21.4% (P < 0.0001). The increment was 7.5% greater for the %FLV compared to that of the %LV (P < 0.001).
Conclusions
The 99mTc-GSA scintigraphy SPECT–CT fusion system can estimate the correct functional liver volume and is useful in comparison with conventional CT volumetry.




Similar content being viewed by others

Abbreviations
- HCC:
-
Hepatocellular carcinoma
- PVE:
-
Portal vein embolization
- %LV:
-
Percentage of non-tumorous remnant liver volume
- %FLV:
-
Percentage of functional remnant liver volume
- SPECT:
-
Single-photon emission computed tomography
- 99mTc-GSA scintigraphy:
-
99mTc-galactosyl human serum albumin scintigraphy
- LHL 15:
-
Uptake ratio of the liver to the liver plus heart at 15 min
- ICG R15:
-
Indocyanine green retention rate at 15 min
References
Wei AC, Poon RT, Fan ST, Wong J. Risk factors for perioperative morbidity and mortality after extended hepatectomy for hepatocellular carcinoma. Br J Surg. 2003;90:33–41.
Vauthey JN, Pawlik TM, Abdalla EK, Arens JF, Nemr RA, Wei SH, et al. Is extended hepatectomy for hepatobiliary malignancy justified? Ann Surg. 2004;239:722–30.
Nagino M, Kamiya J, Nishio H, Ebata T, Arai T, Nimura Y. Two hundred forty consecutive portal vein embolizations before extended hepatectomy for biliary cancer: surgical outcome and long-term follow-up. Ann Surg. 2006;243:364–72.
Yamanaka J, Saito S, Fujimoto J. Impact of preoperative planning using virtual segmental volumetry on liver resection for hepatocellular carcinoma. World J Surg. 2007;31:1249–55.
Schindl MJ, Redhead DN, Fearon KC, Garden OJ, Wigmore SJ. The value of residual liver volume as a predictor of hepatic dysfunction and infection after major liver resection. Gut. 2005;54:289–96.
Makuuchi M, Thai BL, Takayasu K, Takayama T, Kosuge T, Gunve′n P, et al. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery. 1990;107:521–7.
Abdalla EK, Hicks ME, Vauthey JN. Portal vein embolization: rationale, technique and future prospects. Br J Surg. 2001;88:165–75.
Beppu T, Iwatsuki M, Okabe H, Okabe K, Masuda T, Hayashi H, et al. A new approach to percutaneous transhepatic portal embolization using ethanolamine oleate iopamidol. J Gastroenterol. 2010;45:211–7. Epub 2009 Oct 10.
Mitsumori A, Nagaya I, Kimoto S, Akaki S, Togami I, Takeda Y, et al. Preoperative evaluation of hepatic functional reserve following hepatectomy by technetium-99m galactosyl human serum albumin liver scintigraphy and computed tomography. Eur J Nucl Med. 1998;25:1377–82.
Kubo S, Shiomi S, Tanaka H, Shuto T, Takemura S, Mikami S et al. Evaluation of the effect of portal vein embolization on liver function by (99m) Tc-galactosyl human serum albumin scintigraphy. J Surg Res. 2002;107:113–8.
Hirai I, Kimura W, Fuse A, Suto K, Urayama M, et al. Evaluation of preoperative portal embolization for safe hepatectomy, with special reference to assessment of nonembolized lobe function with 99mTc-GSA SPECT scintigraphy. Surgery. 2003;133(5):495–506.
Nanashima A, Yamaguchi H, Shibasaki S, Morino S, Ide N, Takeshita H, et al. Relationship between CT volumetry and functional liver volume using technetium-99m galactosyl serum albumin scintigraphy in patients undergoing preoperative portal vein embolization before major hepatectomy: a preliminary study. Dig Dis Sci. 2006;51:1190–5.
Kwon AH, Matsui Y, Kaibori M, Ha-Kawa SK. Preoperative regional maximal removal rate of technetium-99m-galactosyl human serum albumin (GSA-Rmax) is useful for judging the safety of hepatic resection. Surgery. 2006;140:379–86.
Okabe K, Beppu T, Masuda T, Hayashi H, Okabe H, Komori H et al. Portal vein embolization can prevent intrahepatic metastases to non-embolized liver. Hepatogastroenterology (in press).
Utsunomiya D, Tomiguchi S, Shiraishi S, Yamada K, Honda T, Kawanaka K, et al. Initial experience with X-ray CT based attenuation correction in myocardial perfusion SPECT imaging using a combined SPECT/CT system. Ann Nucl Med. 2005;19:485–9.
Shiraishi S, Tomiguchi S, Utsunomiya D, Kawanaka K, Awai K, Morishita S, et al. Quantitative analysis and effect of attenuation correction on lymph node staging of non-small cell lung cancer on SPECT and CT. AJR Am J Roentgenol. 2006;186:1450–7.
Paugam-Burtz C, Janny S, Delefosse D, Dahmani S, Dondero F, Mantz J, et al. Prospective validation of the “fifty-fifty” criteria as an early and accurate predictor of death after liver resection in intensive care unit patients. Ann Surg. 2009;249:124–8.
Tashiro S. Mechanism of liver regeneration after liver resection and portal vein embolization (ligation) is different? J Hepatobiliary Pancreat Surg. 2009;16:292–9.
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Beppu, T., Hayashi, H., Okabe, H. et al. Liver functional volumetry for portal vein embolization using a newly developed 99mTc-galactosyl human serum albumin scintigraphy SPECT–computed tomography fusion system. J Gastroenterol 46, 938–943 (2011). https://doi.org/10.1007/s00535-011-0406-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-011-0406-x