
Abstract
Infants born at term requiring mechanical ventilation suffer significant mortality and morbidity, yet few studies have tried to identify the optimum respiratory support for such infants. We, therefore, hypothesised that practice would vary, particularly between different levels of neonatal care provision. The lead clinicians of all 212 UK neonatal units were asked to complete an electronic web-based survey regarding respiratory support practices for term-born infants. Survey questions included the level of neonatal care provided, number of term-born infants ventilated per annum, initial and rescue ventilation modes and whether surfactant or inhaled nitric oxide (NO) were used. The overall response rate was 82 %. A greater proportion of neonatal intensive care units (NICUs) compared to local neonatal units (LNUs) stated that they used volume-targeting, particularly for infants with RDS (p = 0.0006) or congenital pneumonia (p = 0.0005). High-frequency oscillatory ventilation was stated as initial mode by a greater proportion of NICUs compared to LNUs and special care units (SCUs), particularly for respiratory distress syndrome (p < 0.0001) or persistent pulmonary hypertension of the newborn (p < 0.001). Continuous mandatory ventilation was stated to be the rescue mode by a greater proportion of LNUs/SCUs compared to NICUs (p < 0.0001). Surfactant was stated to be most commonly given for respiratory distress syndrome (79 % of units) and MAS (61 % of units); surfactant use was lowest in SCUs (p < 0.0001); inhaled NO was infrequently used by LNUs and SCUs. Conclusions There was considerable variation in respiratory support practices for term-born infants, particularly between different levels of neonatal care provision.
Similar content being viewed by others


Introduction
It has been estimated that 3.6 per 1,000 infants born at term (37–41 weeks of gestational age) require mechanical ventilation [8]. Such infants have a high mortality rate ranging from 9.1 % to 12.2 % [2, 13, 18]. Congenital anomalies are a contributing factor [2, 13], but in one study [18], a mortality rate of 9.6 % to 12.2 % was reported in term-born infants without major congenital anomalies. Ventilated, term-born infants can also suffer considerable morbidity. In one study [8], 5 % of the infants developed chronic lung disease, 7 % developed neurological complications and 24 % developed pneumothoraces. There have, however, been few studies attempting to identify the optimum mode of respiratory support in term-born infants. In the UK, there are three levels of neonatal care provided [3]: Special care units (SCU) provide special care for their own local population, local neonatal units (LNU) provide special and high dependency care and a restricted volume of intensive care (as agreed locally), and neonatal intensive care units (NICU) are larger intensive care units that provide the whole range of medical (and sometimes surgical) neonatal care. SCUs and LNUs should transfer infants with ongoing complex respiratory support requirements to NICUs. Hence, it seemed likely that practice would vary, particularly between different levels of neonatal care. In addition, given the lack of evidence, we hypothesised that respiratory support practices used for term-born infants might reflect evidence from studies of prematurely born infants. The aim of this study was to test those hypotheses by carrying out a survey of neonatal units in the UK to document current respiratory support practices in term-born infants.
Materials and methods
Lead clinicians of all 212 neonatal units in the UK were identified from the BLISS directory and contact details confirmed by contacting each hospital. Clinicians were sent an email inviting them to complete an electronic web-based survey (Appendix A) from May to July 2011. The survey included questions on the level of neonatal care provided by the hospital, the number of term newborns ventilated per annum and the type of ventilator used. Practitioners were also asked which ventilation mode was used initially and as rescue mode for various conditions and if they extubated infants directly from high-frequency oscillatory ventilation (HFOV). A question regarding continuous positive airways pressure (CPAP) was included in the survey, as we were interested to determine how many units used CPAP initially rather than ventilation modes and for which diagnoses. They were also asked what level of volume-targeting was used and whether surfactant and inhaled nitric oxide (iNO) were administered.
Analysis
Differences in the responses between practitioners from different levels of neonatal care were assessed for statistical significance using the chi-square test.
Results
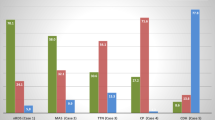
The response rate was 82 %. Practitioners from 90 % of NICUs (57 of 63 NICUs), 96 % of LNUs (80 of 83 LNUs) and 56 % of SCUs (37 of 66 SCUs) responded. Per annum, most NICUs and LNUs ventilated between 10 and 50 term-born infants, 42 % of NICUs ventilated more than 50 term-born infants, whereas 68 % of SCUs ventilated less than ten term-born infants (Fig. 1).

Number of term-born infants per annum by level of neonatal care
The three most frequently used ventilators for conventional ventilation, which is other than HFOV, were the SLE 5000, SLE 2000 (SLE Ltd., South Croydon, UK) and the Dräger Babylog 8000 or 8000plus (Dräger Medical, Lübeck, Germany); many units used more than one type of ventilator. HFOV was provided by all NICUs; several units used more than one type of oscillator: 49 % used the SLE 5000, 47 % the Sensormedics 3100A (CareFusion, San Diego, CA, USA) and 18 % the Stephanie (F. Stephan GmbH, Gackenbach, Germany).
It was reported that 26 % of NICUs and 11 % of LNUs used volume-targeted ventilation (VTV) routinely in term-born infants. A greater proportion of NICUs stated that they used VTV compared to LNUs as the initial ventilation mode, particularly for infants with RDS (p = 0.0006) or congenital pneumonia (p = 0.0005) (Table 1). A wide variety of volume-target levels (3–10 ml/kg) were stated to be used. In both NICUs and LNUs, the volume-targeted level was weaned before extubation to a median of 4 ml/kg, range 3–5 ml/kg. HFOV was stated to be used as the initial ventilation mode by a greater proportion of NICUs compared to LNUS and SCUs for meconium aspiration syndrome (p = 0.044) or persistent pulmonary hypertension of the newborn (p = 0.001) (Table 1). Conventional mechanical ventilation (CMV) was stated to be used as rescue mode by a greater proportion of LNUs compared to NICUs (p < 0.001), whereas HFOV was stated to be used as rescue mode by a greater proportion of NICUs compared to LNUs (p < 0.0001) (Table 2). The majority of SCUs stated that any infant requiring rescue support would be transferred to a unit providing a higher level of neonatal care. In 61 % of NICUs, infants were changed from HFOV to conventional ventilation prior to extubation, whereas in the other 39 % of units, infants were extubated directly from HFOV.
CPAP was used in a number of units, most commonly for infants with RDS (Table 1). For other respiratory conditions, CPAP was used more commonly in LNUs and SNUs. Pressure support ventilation was rarely used.
It was reported that surfactant was given in 61 % of units for infants with MAS and in 79 % of units for infants with RDS. The use of surfactant for different conditions did not differ significantly between different levels of care, except that surfactant was less likely to be given in SCUs than NICUs or LNUs for infants with RDS (p < 0.0001) (Fig. 2). Too few of the LNUs or SCUs stated that they used nitric oxide to all meaningful analysis of their results. In 55 % of NICUs, nitric oxide was stated to be started at 20 ppm, in 25 % at 10 ppm and in 20 % at 5 ppm. In 76 % of NICUs, the maximum dose was stated to be 20 ppm, in 4 % 25 ppm and in 20 % 40 ppm.

Use of surfactant by diagnosis and level of neonatal care
Discussion
These results demonstrate that there was significant variation in respiratory support practices between hospitals providing different levels of neonatal care. This, in part, reflects that in line with the BAPM guidelines [3], SCUs and LNUs (to a lesser extent) transfer infants requiring rescue respiratory support to a unit providing a higher level of neonatal care. There were, however, variations in practice between NICUs, for example different levels of volume-targeting and different starting doses of iNO were used. There have been relatively few studies which have investigated respiratory support for term-born infants. The results of our survey also highlight that even where there is an evidence base, not all units have implemented such evidence (see the following discussion).
A recent survey of 173 European neonatal units highlighted that in a predominately prematurely born population, 85 % of patients were conventionally ventilated [19], whereas the results of another survey demonstrated that 60 % of Australasian NICUs and 40 % of Scandinavian NICUs routinely used VTV in prematurely born infants [11]. The latter survey's results perhaps reflect the positive benefits reported in prematurely born infants in the recent Cochrane Review [21]. We now demonstrate that 26 % of UK NICUs routinely use VTV in term-born infants, although there have been no randomised studies demonstrating similar benefits in term-born infants. Practitioners stated that they used volume-target levels from 3 to 10 ml/kg with the median minimum volume-target level used prior to extubation of 4 ml/kg. In term-born infants with acute respiratory distress, we have recently demonstrated that a VT level of 6 ml/kg rather than 4 ml/kg reduces the work of breathing [4].
A variety of ventilators were used for both conventional and high-frequency oscillatory ventilation. We have previously shown [17] that during VTV, different types of ventilators deliver different airway pressure waveforms, but whether this influences outcome has not been tested. Only 47 % of units stated that they used the Sensormedics for term-born infants. Oscillator performance also differs [12], with the Sensormedics delivering greater tidal volumes, particularly at lower frequencies compared to the Draeger and SLE ventilators in oscillator mode
For term-born infants, there is no evidence to support the use of prophylactic HFO and little evidence to support use of HFO in infants with severe pulmonary dysfunction born at or near term [9]. In a meta-analysis [9] of two randomised trials comparing HFOV to conventional ventilation (CV), no reductions in mortality at 28 days, pulmonary air leak, chronic lung disease (28 days or more in oxygen) or intracranial injury were demonstrated. In the one rescue study [5] included in the meta-analysis [9], there was no difference in the risk of needing extracorporeal membrane oxygenation (ECMO). Despite the paucity of evidence, the results of this survey demonstrated that many practitioners from NICUs indicated that they used HFOV as rescue mode. As their respiratory failure improves, infants on HFOV can be switched either to CMV for further weaning prior to extubation or be extubated directly from HFOV. There is no evidence to determine whether one method is better than the other for term-born infants, yet the majority of practitioners from NICUs stated that they changed infants to CMV from HFOV for a period prior to extubation.
There is evidence to support surfactant use in certain respiratory conditions in term-born infants. In meconium aspiration syndrome in infants born at or near term, a meta-analysis demonstrated that surfactant reduced the risk of requiring ECMO (relative risk (RR) 0.64, 95 % confidence interval (CI) 0.46, 0.91) [6]. A randomised, multicentre, double-blind, placebo-controlled trial in term infants with severe respiratory failure due to MAS, sepsis or idiopathic PPHN demonstrated that administration of surfactant was associated with a significant reduction in the need for ECMO (p = 0.038), but no statistically significant difference in the duration of ventilation or the incidence of chronic lung disease [14]. A retrospective observational study [10] of 118 infants with respiratory failure and group B streptococcal infection, 19 % of whom were more than 35-week gestation, showed a significant reduction in the median fraction of inspired oxygen (FiO2) with surfactant treatment (0.84 to 0.5, p < 0.01). Observational studies, mostly in prematurely born infants with pulmonary haemorrhage, have shown that surfactant administration was associated with an improvement in the severity of respiratory failure [1] and a significant reduction in the mean oxygenation index [16]. No benefit, however, has been shown in administering surfactant to term-born infants with congenital diaphragmatic hernia (CDH). Indeed, in antenatally diagnosed, term-born, CDH patients, surfactant treatment was associated with a higher use of ECMO (p = 0.04), a higher incidence of chronic lung disease (p = 0.0066) and a lower survival rate (p = 0.0033) [20].
Inhaled NO reduces the incidence of the combined outcome of death or need for ECMO in ventilated, term-born infants [7]. A review of four studies highlighted that the maximal beneficial effect of NO occurs at less than 30 ppm [15]; as a consequence, it has been recommended that the starting dose should be 20 ppm [7]. The results of this survey demonstrated that practitioners from only 55 % of NICUs stated that they were using a starting dose of 20 ppm [7].
A limitation of this study is that we approached a single practitioner from each of the units to complete the questionnaire. It may be that they responded with their personal views, but they were identified as the lead clinicians, and their views represent practitioners from different levels of neonatal care provision. Although practitioners from 90 % of NICUs and 96 % of LNUs responded to survey, the response rate from practitioners from SCUs was much lower (56 %). We do not, however, feel that this significantly affected our findings as SCUs provide only special care for their local population and should transfer infants with ongoing complex respiratory support requirements to NICUs [3]. Indeed, the majority of SCUs stated that any infant requiring rescue support would be transferred to a unit providing a higher level of neonatal care.
In conclusion, we have shown that there is considerable variation in respiratory support practice for term-born infants, particularly between practitioners from units offering different levels of neonatal care. These results emphasise that further research is required to produce evidence-based guidelines for the respiratory support of term-born infants.
References
Amizuka T, Shimizu H, Niida Y, Ogawa Y (2003) Surfactant therapy in neonates with respiratory failure due to haemorrhagic pulmonary oedema. Eur J Pediatr 162:697–702
Angus DC, Linde-Zwirble WT, Clermont G, Griffin MF, Clark RH (2001) Epidemiology of neonatal respiratory failure in the United States: projections from California and New York. Am J Respir Crit Care Med 164:1154–1160
British Association of Perinatal Medicine (2010) Service standards for hospitals providing neonatal care (3rd Edition)
Chowdhury O, Patel DS, Sharma A, Prendergast M, Rafferty GF, Greenough A (2011) Volume-targeted ventilation in infants born at or near term. Arch Dis Child Fetal Neonatal Ed [Epub ahead of print]
Clark RH, Yoder BA, Sell MS (1994) Prospective, randomized comparison of high-frequency oscillation and conventional ventilation in candidates for extracorporeal membrane oxygenation. J Pediatr 124:447–454
El Shahed AI, Dargaville P, Ohlsson A, Soll RF (2007) Surfactant for meconium aspiration syndrome in full term/near term infants. Cochrane Database Syst Rev 3:CD002054
Finer NN, Barrington KJ (2006) Nitric oxide for respiratory failure in infants born at or near term. Cochrane Database Syst Rev 4:CD000399
Gouyon JB, Ribakovsky C, Ferdynus C, Quantin C, Sagot P, Gouyon B, Network BP (2008) Severe respiratory disorders in term neonates. Paediatr Perinat Epidemiol 22:22–30
Henderson-Smart DJ, De Paoli AG, Clark RH, Bhuta T (2009) High frequency oscillatory ventilation versus conventional ventilation for infants with severe pulmonary dysfunction born at or near term. Cochrane Database Syst Rev 3:CD002974
Herting E, Henderson-Smart DJ, De Paoli AG, Clark RH, Bhuta T (2000) Surfactant treatment of neonates with respiratory failure and group B streptococcal infection. Members of the Collaborative European Multicenter Study Group. Pediatrics 106:957–964
Klingenberg C, Wheeler KI, Owen LS, Kaaresen PI, Davis PG (2011) An international survey of volume-targeted neonatal ventilation. Arch Dis Child Fetal Neonatal Ed 96:F146–F148
Laubscher B, Greenough A, Costeloe K (1996) Performance of four neonatal high frequency oscillators. Br J Intens Care 6:148–152
Lian WB, Yeo CL, Ho LY (2002) Two-year outcome of normal-birth-weight infants admitted to a Singapore neonatal intensive care unit. Ann Acad Med Singap 31:199–205
Lotze A, Mitchell BR, Bulas DI, Zola EM, Shalwitz RA, Gunkel JH (1998) Multicenter study of surfactant (beractant) use on the treatment of term infants with severe respiratory failure. Survanta in Term Infants Study Group. J Pediatr 132:40–47
Macrae DJ, Field D, Mercier JC, Møller J, Stiris T, Biban P, Cornick P, Goldman A, Göthberg S, Gustafsson LE, Hammer J, Lönnqvist PA, Sanchez-Luna M, Sedin G, Subhedar N (2004) Inhaled nitric oxide therapy in neonates and children: reaching a European consensus. Intensive Care Med 30:372–380
Pandit PB, Dunn MS, Colucci EA (1995) Surfactant therapy in neonates with respiratory deterioration due to pulmonary hemorrhage. Pediatrics 95:32–36
Sharma A, Milner AD, Greenough A (2007) Performance of neonatal in ventilators in volume targeted ventilation mode. Acta Paediatr 96:176–180
Sutton L (1997) Population-based data on full-term neonates with severe morbidity. Semin Neonatol 2:189–193
Van Kaam AH, Rimensberger PC, Borensztajn D, De Jaegere AP, on behalf of the Neovent Study Group (2010) Ventilation practices in the neonatal intensive care unit: a cross-sectional study. J Pediatr 157:767–771
Van Meurs K (2004) Is surfactant therapy beneficial in the treatment of the term newborn infant with congenital diaphragmatic hernia? J Pediatr 145:312–316
Wheeler K, Klingenberg C, McCallion N, Morley CJ, Davis PG (2010) Volume-targeted versus pressure-limited ventilation in the neonate. Cochrane Database Syst Rev 11:CD003666
Acknowledgements
Dr. Chowdhury is supported by the Charles Wolfson Charitable Trust. We would like to thank Mrs. Deirdre Gibbons for the secretarial assistance.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(PDF 222 kb)
Rights and permissions
About this article
Cite this article
Chowdhury, O., Wedderburn, C.J., Lee, S. et al. Respiratory support practices in infants born at term in the United Kingdom. Eur J Pediatr 171, 1633–1638 (2012). https://doi.org/10.1007/s00431-012-1784-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-012-1784-7