
Abstract
Background and purpose
During the COVID-19 outbreak, the presence of extensive white matter microhemorrhages was detected by brain MRIs. The goal of this study was to investigate the origin of this atypical hemorrhagic complication.
Methods
Between March 17 and May 18, 2020, 80 patients with severe COVID-19 infections were admitted for acute respiratory distress syndrome to intensive care units at the University Hospitals of Strasbourg for whom a brain MRI for neurologic manifestations was performed. 19 patients (24%) with diffuse microhemorrhages were compared to 18 control patients with COVID-19 and normal brain MRI.
Results
The first hypothesis was hypoxemia. The latter seemed very likely since respiratory failure was longer and more pronounced in patients with microhemorrhages (prolonged endotracheal intubation (p = 0.0002), higher FiO2 (p = 0.03), increased use of extracorporeal membrane oxygenation (p = 0.04)). A relevant hypothesis, the role of microangiopathy, was also considered, since patients with microhemorrhages presented a higher increase of the D-Dimers (p = 0.01) and a tendency to more frequent thrombotic events (p = 0.12). Another hypothesis tested was the role of kidney failure, which was more severe in the group with diffuse microhemorrhages (higher creatinine level [median of 293 µmol/L versus 112 µmol/L, p = 0.04] and more dialysis were introduced in this group during ICU stay [12 versus 5 patients, p = 0.04]).
Conclusions
Blood–brain barrier dysfunction secondary to hypoxemia and high concentration of uremic toxins seems to be the main mechanism leading to critical illness-associated cerebral microbleeds, and this complication remains to be frequently described in severe COVID-19 patients.
Similar content being viewed by others

Introduction
Recently, some cerebral complications related to COVID-19 were depicted on brain MRIs. Diffuse microbleeds, located in the white matter (WM) with an atypical distribution affecting, in particular, the corpus callosum, has recently been described in critically ill patients with COVID-19 [1,2,3,4,5,6,7,8,9]. A recent neuropathological study has also described hemorrhagic lesions disseminated throughout cerebral WM in a patient with severe COVID-19 [10]. Another pathological study [11] described the autopsies of six patients with COVID-19, and among them, four presented diffuse petechial hemorrhages in the brain. These observations can be paralleled with the «critical illness-associated cerebral microbleeds (CIAM)» described in a 10 year follow-up on 12 patients [12].
However, the underlying pathophysiological mechanisms leading to diffuse microbleeds in the COVID-19 pandemic context remain unknown. As summarized in Table 1, several hypotheses were proposed, notably those concerning the potential role of hypoxemia, microangiopathy, or coagulopathy. Our aim in this study is to discuss and address the origin of this atypical hemorrhagic complication in the context of COVID-19, by studying in particular, the three main mechanisms above-mentioned.
Material and methods
This retrospective monocentric study was approved by the ethical committee of Strasbourg University Hospital (CE-2020–37) and was in accordance with the 1964 Helsinki Declaration and its later amendments. Informed consents were waived.
Patient cohort
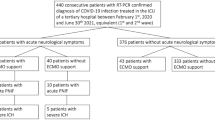
Between March 17 and May 18, 2020, 80 patients with severe COVID-19 infections were admitted for acute respiratory distress syndrome (ARDS) to intensive care units (ICUs) at the University Hospitals of Strasbourg. A cerebral MRI was performed to explain the neurologic manifestations. The diagnosis of COVID-19 was validated with the detection of SARS-CoV-2 by reverse transcriptase–polymerase chain reaction (RT-PCR) assays on upper or lower respiratory tract swabs.
Brain MRI interpretation
All MR studies were performed on a 3 T MR scanner, and all patients performed a 3-dimensional susceptibility-weighted imaging sequence with phase mapping. A standardized imaging protocol was made including in addition: 3D T1-weighted spin-echo MRI with and without contrast enhancement, diffusion-weighted imaging, dynamic susceptibility contrast MR perfusion, 3D FLAIR after administration of gadolinium-based contrast agent, and delayed post-contrast FLAIR.
All brain MRIs were retrospectively reviewed independently by two neuroradiologists (S.K, and F.L. with 20 and 9 years of experience in neuroradiology), who reached a consensus concerning the final diagnosis.
The diagnosis of CIAM was made when brain MRIs showed diffuse brain microhemorrhages, which predominantly involved the corpus callosum (especially the genu and the splenium of the corpus callosum), the subtentorial juxtacortical WM, the internal capsule, the brainstem, the middle cerebellar peduncles, and the cerebellum. The cortex, the basal ganglia, and the thalamus were spared.
In our study, the involvements of the corpus callosum, internal capsule, and middle cerebellar peduncles were mandatory for the diagnosis of CIAM.
The main differential diagnoses were: cerebral amyloid angiopathy (but the extensive corpus callous involvement was atypical, and none of the patients showed cortical superficial siderosis), chronic hypertension (yet the grey matter was spared), and diffuse axonal injury (however, none of our patients had a history of head injury).
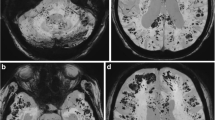
Among the 80 patients above-mentioned, 19 (24%) presented diffuse microhemorrhages located in the WM (Fig. 1), compatible with CIAM.

Susceptibility-weighted MR images in four different critically ill COVID-19 patients: a–c: diffuse microhemorrhages in a 66-year-old man appearing as multiple small hypointense foci within the brainstem and cerebellum (a), the splenium of the corpus callosum (arrowheads) and the internal capsules (arrows) (b), the juxtacortical white matter (c). d, e: Juxtacortical hematomas (arrows) associated with diffuse microhemorrhages in men of 60 (d) and 67 years (e). f subarachnoid hemorrhages (arrows) associated with diffuse microhemorrhages in a 57-year-old man.
Study design
We retrospectively compared these 19 patients to 18 other ICU patients with COVID-19, similar ARDS, and neurological manifestations, but with a normal cerebral MRI, to understand the underlying pathophysiological mechanisms. The control group's brain MRIs were normal, except for leptomeningeal enhancement, common findings during the COVID-19 outbreak, and present in seven patients in the control group and six patients in the CIAM group. Clinical and laboratory data were extracted from the patients’ electronic medical records in the Hospital Information System. Clinical and biological data were reviewed by neurologists and intensivists. The laboratory findings were analyzed at the time of admission to the ICU and during ICU stay before brain MRI. In this latter situation, the worst value has been kept in the case of redundancy of the tests.
According to the Berlin definition [13], all patients had an ARDS, and, therefore, a PaO2/FiO2 ratio of less than 300 mmHg. The severity of an ARDS is further sub-classified into mild (PaO2/FiO2 200 to 300 mmHg), moderate (PaO2/FiO2 100 to 200 mmHg), and severe (PaO2/FIO2 ≤ 100 mm Hg) [13]. The severity of ARDS was also evaluated in our study by the higher inspiratory oxygen fraction (FiO2) delivered during ICU stay, by the number of days intubated, and by the requirement or not of extracorporeal membrane oxygenation (ECMO). Moreover, we evaluated the percentage of lung involvement in chest computed tomography with a numeric scale: 0, 1 (< 10%), 2 (10–25%), 3 (25–50%), 4 (50–75%), 5 (> 75%) [14].
Statistical analysis
Data were described using frequency and proportion (n, %) for categorical variables, using median, first and third quartile, and range for quantitative data.
Categorical data were compared using Fisher exact test. Quantitative data were compared using Mann–Whitney–Wilcoxon test. A p value lower than 0.05 was considered significant.
Results
The clinical features are summarized in Table 2.
Among the 19 patients with a diagnosis of CIAM, some of them were associated with other hemorrhagic complications, such as subarachnoid hemorrhages (5/19, 26%), and intracerebral hematomas (4/19, 21%) (Fig. 1). Five patients presented with convexal subarachnoid hemorrhage, as described in Fig. 1. The bleedings were localized to the brain's convexities with preferential frontal lobe involvement, usually multiple and bilateral, without extension into basal cisterns. Venous structures were excluded by the hyperintensities seen with FLAIR MR imaging.
Four patients presented with intracerebral hematomas, unique in three cases and multiple for one patient. Their maximum sizes for each patient were 2.3 cm, 2.5 cm, 2.7 cm, and 7.7 cm.
Neurologic manifestations (Table 2)
Even if both groups demonstrated a high prevalence of pathological wakefulness when the sedative therapies were stopped, the neurological status seemed more severe in case of extensive WM microhemorrhages: indeed, this group showed more impaired consciousness (p = 0.0006), whereas the second group was associated with less severe clinical signs such as confusion (p = 0.02) and agitation (p = 0.04). Four patients in the CIAM group had seizures, and among them, two also had subarachnoid hemorrhages, and one had a more extensive intracerebral hematoma.
Hypoxemia hypothesis (Table 3)
During ICU stay, before brain MRI, patients with CIAM showed a more severe respiratory status in comparison with those with a normal brain MRI. In fact, these patients required prolonged endotracheal intubation (median of 24 days versus 8 days, p = 0.002) for a more severe ARDS, as evidenced by a tendency in a lower PaO2/FiO2 (median of 81 mmHg versus 104 mmHg, p = 0.07), a higher FiO2 (median of 100% versus 75%, p = 0.03), and increased use of ECMO (5 patients versus 0, p = 0.04) during their stay. Similarly, the pulmonary involvement on chest computed tomography was more severe in the group with diffuse WM microhemorrhages (p = 0.04).
Microangiopathy–microthrombi hypothesis (Tables 2 and 4)
The two groups did not differ concerning the distribution of cardiovascular risk factors. A significant proportion of our patients were at least classified as overweight (first quartile of 26 kg/m2 in the two groups).
At the ICU admission time, the D-dimers levels were higher in the group with diffuse microhemorrhages (median of 3.1 mg/L versus 1.7 mg/L, p = 0.01). A similar trend was observed during ICU stay (higher D-dimers levels of 11.5 mg/L versus 4.6 mg/L, p = 0.08).
There seemed to be more thrombotic events (7 versus 2 patients, p = 0.12), and a higher CRP level (median of 276 mg/L versus 196 mg/L, p = 0.09) during ICU stay in the group with CIAM.
The percentage of positive specimens for lupus anticoagulant was close in both groups (79% versus 83%, p = 1).
Disseminated intravascular coagulation hypothesis
According to the criteria endorsed by the International Society on Thrombosis and Haemostasis [15], only one case of disseminated intravascular coagulation was present in the group with CIAM, and two cases in the second group (p = 0.6). The other coagulation biomarkers were strictly comparable between both groups at the time of admission and during ICU stay, and all patients received anticoagulant therapy during hospitalization.
Other results
The kidney failure was more severe in the group with diffuse microhemorrhages, as evidenced by a higher creatinine level (median of 293 µmol/L versus 112 µmol/L, p = 0.04) and more dialysis were introduced in this group during ICU stay (12 versus 5 patients, p = 0.04).
The two groups were comparable concerning the use of hydroxychloroquine or lopinavir/ritonavir.
Cerebrospinal fluid (CSF) analysis (Table 5)
10 patients underwent a lumbar puncture in the first group and 14 in the second group. The two populations were strictly comparable, and only one patient demonstrated the presence of SARS-CoV-2 on RT-PCR in the control group. In 60% of cases of CIAM, oligoclonal IgG bands identical in serum and CSF (type IV) were present.
Discussion
Since the discovery of cerebral microhemorrhages in patients with COVID-19, several assumptions have been made about the pathogenesis of CIAM listed in Table 1; the presence of cerebral microhemorrhages is a bad-known indicator and reports in patients with severe COVID-19 in imaging [1,2,3,4,5,6,7,8,9], and neuropathological studies [10, 11] increased steadily.
The goal of this study was to evaluate the more likely hypotheses that applied in patients with COVID-19.
Due to the resemblance between CIAM and what is seen in high-altitude cerebral edema [16, 17], the first hypothesis raised concerns hypoxemia. This assumption seems very likely since patients with diffuse microhemorrhages had longer or more pronounced respiratory failure.
Even if the exact mechanisms remain unclear, hypoxemia seems associated with disruptions in the blood–brain barrier, leading to extravasation of erythrocytes. In 30% of the patients for whom a lumbar puncture was realized, their results were consistent with blood–brain barrier disruption (elevated ImmunoglobulinG without a concomitant increase of the Tibbling-link IgG index, and increased albumin quotient).
It is known that ECMO may be associated with brain hemorrhagic complications [18], and the use of ECMO itself may induce, in some cases, diffuse WM microhemorrhages [19]. In our study, five patients diagnosed with CIAM were treated with ECMO and none in the second group. However, it is impossible to say whether these hemorrhagic complications are a specific complication of ECMO or only related to the respiratory state with severe hypoxemia.
The second hypothesis evaluated was the role of microangiopathy. A recent histopathologic study [20], which focused on the pulmonary vessels in patients with COVID-19, described microangiopathy with disseminated microthrombi. This assumption concerning microangiopathy with diffuse microthrombi may also explain the extensive brain microhemorrhages: patients expressed higher D-dimers levels upon ICU admission, tend to have a higher increase in D-dimers, C-reactive protein, and more thromboembolic events during their stay in the ICU.
Nevertheless, the differences between both groups were not pronounced; microthrombi typically cause punctate foci of restricted diffusion on brain MRI scans, which have not been observed in our patients.
The third new hypothesis was formulated based on our results: the role of kidney failure, which was more severe in the group with CIAM. It is known that chronic kidney disease and hemodialysis are associated with a high incidence of microbleeds [21, 22]. The underlying physiological mechanisms including increased permeability of the blood–brain barrier secondary to a high concentration of uremic toxins [21]. Indeed, the group of patients with COVID-19 diagnosed with CIAM have shown a more severe kidney failure in agreement with this new assumption.
A combination of the above assumptions should also be considered, but the number of patients in our cohort does not allow us to test the cross hypotheses. Further studies with more patients and more diversity are needed to test all cases.
Although possible, the hypothesis of coagulation disorders has not been supported by our data to be involved in the development of microbleeds on patients with COVID-19. Only one patient had a diagnosis of disseminated intravascular coagulation in the group CIAM. The other coagulation biomarkers were strictly comparable between both groups at the time of admission and during ICU stay, and all patients received anticoagulant therapy during hospitalization.
In the group CIAM, CSF analysis did not reveal any evidence of direct viral infection of the central nervous system (SARS-CoV-2 RNA was not detected, and no intrathecal synthesis was highlighted).
It is very likely that a significant number of patients with COVID-19-associated ARDS have had and will present this complication. Thereby, the diagnosis of CIAM by MRI is essential, and this entity should be known to avoid misdiagnoses such as hemorrhagic encephalitis related to SARS-CoV-2. Thus, it could have important implications for patients care. However, many uncertainties remain, particularly in regard to long-term prognosis and prevention. In other situations, outside the COVID-19 outbreak, it is recognized that cerebral microbleeds are independently associated with cognitive dysfunction [23]. The prognosis of our patients will also require further long-term follow-up studies.
Data availability
We state that the data published are available and anonymized and will be shared upon request by email to the corresponding author from any qualified investigator for purposes of replicating procedures and results.
Abbreviations
- ARDS:
-
Acute respiratory distress syndrome
- CIAM:
-
Critical illness-associated cerebral microbleeds
- CSF:
-
Cerebrospinal fluid
- ECMO:
-
Extracorporeal Membrane Oxygenation
- ICU:
-
Intensive care unit
- RT-PCR:
-
Reverse transcriptase–polymerase chain reaction
- WM:
-
White matter
References
Radmanesh A, Derman A, Lui YW et al (2020) COVID-19-associated diffuse leukoencephalopathy and microhemorrhages. Radiology. https://doi.org/10.1148/radiol.2020202040 ([published online ahead of print, 2020 May 21])
Kremer S, Lersy F, de Sèze J et al (2020) Brain MRI severe COVID-19: a retrospective observational study. Radiology. https://doi.org/10.1148/radiol.2020202222 ([published online ahead of print, 2020 Jun 16])
Vattoth S, Abdelhady M, Alsoub H, Own A, Elsotouhy A (2020) Critical illness-associated cerebral microbleeds in COVID-19. Neuroradiol J. https://doi.org/10.1177/1971400920939229 ([published online ahead of print, 2020 Aug 6])
Chougar L, Shor N, Weiss N et al (2020) Retrospective observational study of brain magnetic resonance imaging findings in patients with acute SARS-CoV-2 infection and neurological manifestations. Radiology. https://doi.org/10.1148/radiol.2020202422 ([published online ahead of print, 2020 Jul 17])
Klironomos S, Tzortzakakis A, Kits A et al (2020) Nervous system involvement in covid-19: results from a retrospective consecutive neuroimaging cohort. Radiology. https://doi.org/10.1148/radiol.2020202791 ([published online ahead of print, 2020 Jul 30])
Lin E, Lantos JE, Strauss SB et al (2020) Brain imaging of patients with COVID-19: findings at an academic institution during the height of the outbreak in New York City. AJNR Am J Neuroradiol. https://doi.org/10.3174/ajnr.A6793 ([published online ahead of print, 2020 Aug 20])
Paterson RW, Brown RL, Benjamin L et al (2020) The emerging spectrum of COVID-19 neurology: clinical, radiological and laboratory findings. Brain. https://doi.org/10.1093/brain/awaa240 ([published online ahead of print, 2020 Jul 8])
Fitsiori A, Pugin D, Thieffry C, Lalive P, Vargas MI (2020) Unusual microbleeds in brain MRI of Covid-19 patients. J Neuroimaging. https://doi.org/10.1111/jon.12755 ([published online ahead of print, 2020 Jul 8])
Freeman CW, Masur J, Hassankhani A, Wolf RL, Levine JM, Mohan S (2020) COVID-19-related disseminated leukoencephalopathy (CRDL): a retrospective study of findings on brain MRI. AJR Am J Roentgenol. https://doi.org/10.2214/AJR.20.24364 ([published online ahead of print, 2020 Sep 9])
Reichard RR, Kashani KB, Boire NA, Constantopoulos E, Guo Y, Lucchinetti CF (2020) Neuropathology of COVID-19: a spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. https://doi.org/10.1007/s00401-020-02166-2 ([published online ahead of print, 2020 May 24])
von Weyhern CH, Kaufmann I, Neff F, Kremer M (2020) Early evidence of pronounced brain involvement in fatal COVID-19 outcomes. Lancet 395(10241):e109. https://doi.org/10.1016/S0140-6736(20)31282-4
Fanou EM, Coutinho JM, Shannon P et al (2017) Critical illness-associated cerebral microbleeds. Stroke 48(4):1085–1087. https://doi.org/10.1161/STROKEAHA.116.016289
The ARDS Definition Task Force* (2012) Acute respiratory distress syndrome: the Berlin definition. JAMA 307(23):2526–2533. https://doi.org/10.1001/jama.2012.5669
Revel MP, Parkar AP, Prosch H et al (2020) COVID-19 patients and the radiology department—advice from the European Society of Radiology (ESR) and the European Society of Thoracic Imaging (ESTI). Eur Radiol 30(9):4903–4909. https://doi.org/10.1007/s00330-020-06865-y
Taylor FB, Toh CH, Hoots WK, Wada H, Levi M (2001) Scientific subcommittee on disseminated intravascular coagulation (DIC) of the International Society on Thrombosis and Haemostasis (ISTH). Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost. 86(5):1327–1330
Kallenberg K, Dehnert C, Dörfler A et al (2008) Microhemorrhages in nonfatal high-altitude cerebral edema. J Cereb Blood Flow Metab 28(9):1635–1642. https://doi.org/10.1038/jcbfm.2008.55
Schommer K, Kallenberg K, Lutz K, Bärtsch P, Knauth M (2013) Hemosiderin deposition in the brain as footprint of high-altitude cerebral edema. Neurology 81(20):1776–1779. https://doi.org/10.1212/01.wnl.0000435563.84986.78
Xie A, Lo P, Yan TD, Forrest P (2017) Neurologic complications of extracorporeal membrane oxygenation: a review. J Cardiothorac Vasc Anesth 31(5):1836–1846. https://doi.org/10.1053/j.jvca.2017.03.001
Shah J, Armstrong MJ (2015) Extracorporeal membrane oxygenation: uncommon cause of corpus callosal microhemorrhage. Neurology 84(6):630. https://doi.org/10.1212/WNL.0000000000001227
Ackermann M, Verleden SE, Kuehnel M et al (2020) Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in covid-19. N Engl J Med. https://doi.org/10.1056/NEJMoa2015432 ([published online ahead of print, 2020 May 21])
Lau WL, Nunes ACF, Vasilevko V et al (2020) Chronic kidney disease increases cerebral microbleeds in mouse and man. Transl Stroke Res 11(1):122–134. https://doi.org/10.1007/s12975-019-00698-8
Yokoyama S, Hirano H, Uomizu K, Kajiya Y, Tajitsu K, Kusumoto K (2005) High incidence of microbleeds in hemodialysis patients detected by T2*-weighted gradient-echo magnetic resonance imaging. Neurol Med Chir (Tokyo) 45(11):556–560. https://doi.org/10.2176/nmc.45.556
Werring DJ, Frazer DW, Coward LJ et al (2004) Cognitive dysfunction in patients with cerebral microbleeds on T2*-weighted gradient-echo MRI. Brain 127(Pt 10):2265–2275. https://doi.org/10.1093/brain/awh253
Funding
The authors declare no funding source.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Lersy, F., Willaume, T., Brisset, JC. et al. Critical illness-associated cerebral microbleeds for patients with severe COVID-19: etiologic hypotheses. J Neurol 268, 2676–2684 (2021). https://doi.org/10.1007/s00415-020-10313-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-020-10313-8