
Abstract
Patients with an acute basilar artery occlusion (BAO) have a high risk of long-lasting disability and death. Only limited data are available on functional outcome in elderly patients with BAO. Using data from the Basilar Artery International Cooperation Study, we aimed to determine outcomes in patients ≥75 years. Primary outcome measure was poor functional outcome (modified Rankin scale score 4–6). Secondary outcomes were death, insufficient vessel recanalization (defined as thrombolysis in myocardial infarction score 0–1) and symptomatic intracranial hemorrhage (SICH). Patients were divided into four age-groups, based on quartiles: 18–54, 55–64, 65–74, and ≥75 years. Outcomes were compared between patients ≥75 years and patients aged 18–54 years. Risk ratios with corresponding 95 % confidence intervals (CI) were calculated and Poisson regression analyses were performed to calculate adjusted risk ratios (aRR). We included 619 patients [18–54 years n = 153 (25 %), 55–64 years n = 133 (21 %), 65–74 years n = 171 (28 %), and ≥75 years n = 162 (26 %)]. Compared with patients aged 18–54 years, patients ≥75 years were at increased risk of poor functional outcome [aRR 1.33 (1.14–1.55)] and death [aRR 2.47 (1.75–3.51)]. Nevertheless, 35/162 (22 %, 95 % CI 15–28 %) of patients ≥75 years had good functional outcome. No significant differences between age groups were observed for recanalization rate and incidence of SICH. Although patients ≥75 years with BAO have an increased risk of poor outcome compared with younger patients, a substantial group of patients ≥75 years survives with a good functional outcome.
Similar content being viewed by others

Introduction
Patients with an acute basilar artery occlusion (BAO) have a high risk of long-lasting disability and death [1, 2]. Although higher age, analyzed as a continuous variable, has been associated with poor functional outcome after BAO, only limited data are available on functional outcome in elderly patients [3–8]. One small case series suggested that all patients ≥75 years have poor functional outcome [6]. In another study, the eldest surviving patient in whom recanalization was successful was 63-year-old [3]. We analysed data from the Basilar Artery International Cooperation Study (BASICS) to determine outcomes in patients with BAO ≥75 years.
Methods
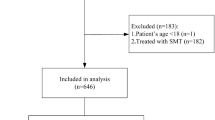
BASICS is a prospective, observational, registry of 619 consecutive patients ≥18 years with an acute symptomatic BAO [2, 9]. The protocol was approved by the ethics committee of the University Medical Center Utrecht, the Netherlands. Embolic BAO was defined as complete recanalization on follow-up and no indication of dissection, or maximum deficit from onset and cardiac or vertebral source of embolism, or maximum deficit from onset with complete absence of other atherosclerotic cerebrovascular lesions. Atherosclerotic BAO was defined as known symptomatic basilar artery stenosis (>50 %) prior to occlusion, or residual stenosis after recanalization and no evidence of cardiac or vertebral artery source of embolism, or prior TIAs or stroke in the basilar artery territory and no evidence of cardiac or vertebral artery source of embolism. Dissections were not predefined, but scored according to the investigators.
Primary outcome was poor functional outcome after 1 month [predefined as modified Rankin scale (mRS) score 4–6]. Secondary outcomes were death, insufficient vessel recanalization [defined as thrombolysis in myocardial infarction (TIMI) score 0–1] and symptomatic intracranial hemorrhage (SICH). We also investigated if our conclusions changed if poor functional outcome was defined as an mRS of 3–6. SICH was not predefined by the registry, and the reporting of SICH was done on the basis of each investigator’s judgment. For the purpose of this study, patients were divided into four age-groups, based on quartiles: 18–54, 55–64, 65–74, and ≥75 years. Outcomes were compared between patients ≥75 years and patients aged 18–54 years. Risk ratios (RR) and corresponding 95 % confidence intervals (CI) were calculated. Variables that affected the crude risk ratio most were used simultaneously in Poisson regression analyses to calculate adjusted risk ratios (aRR) [2]. Missing baseline data (<5 % for each variable) were imputed with regression imputation [10]. Finally, we explored the incidence of poor functional outcome in patients 75–79, 80–84, 85–89, and 90 years or older.
Results
Baseline characteristics are listed in Table 1. In total, 162 patients (26 % of total cohort) were ≥75 years. In this group of patients, the most common cause of stroke was embolism and 64 % had an NIHSS score >20. Treatment of any kind was initiated in 148 patients (91 %).
Modified Rankin Scale scores for all age groups are presented in Fig. 1. Patients ≥75 years had a higher risk of poor functional outcome [aRR 1.33 (1.14–1.55), Table 2] and death [aRR 2.47 (1.75–3.51), Table 3] than patients aged 18–54 years. Nevertheless, 35 patients (22 %, 95 % CI 15–28 %) of those ≥75 years had a good functional outcome. No significant differences between age groups were observed for insufficient recanalization [patients ≥75 vs. 18–54 years aRR 1.69 (0.95–3.03)] and SICH [patients ≥75 vs. 18–54 years RR 1.77 (0.77–4.06)]. Since SICH occurred in only 42 (7 %) patients, no further analyses were performed for this outcome measure.

Modified Rankin scale scores according to age group. mRS modified Rankin scale score
If poor functional outcome was defined as an mRS of 3–6, the proportion of patients with poor functional outcome in each age group was 108/153 (71 %) in patients 18–54 years of age, 101/133 (76 %) in patients 55–64 years, 142/171 (83 %) in patients 65–74 years, and 137/162 (85 %) in patients ≥75 years. Also when this definition was used, patients ≥75 years had a higher risk of poor functional outcome [aRR 1.21 (1.07–1.36)] than patients aged 18–54 years.
Baseline characteristics of patients ≥75 years and their relationship with functional outcome are shown in Table 4. The following variables were associated with an increased risk of poor functional outcome after 1 month: male sex (RR 1.18, 95 % CI 1.00–1.38), location of occlusion (middle third vs. distal third: RR 1.21, 95 % CI 1.02–1.44), NIHSS score >20 on presentation (RR 1.36, 95 % CI 1.10–1.67), type of treatment (no treatment vs. intra-arterial thrombolytic therapy (IAT) only: RR 1.32, 95 % CI 1.15–1.52), SICH (RR 1.21, 95 % CI 1.03–1.43), and insufficient recanalization (RR 1.38, 95 % CI 1.07–1.77).
The proportion of patients with poor functional outcome in age subgroups ≥75 years was as follows: 64/82 (78 %) in patients 75–79 years of age, 40/49 (82 %) in patients 80–84 years, 16/23 (70 %) in patients 85–89 years, and 7/8 (88 %) in patients 90 years or older. The oldest patient with good functional outcome was 91 years of age, despite an NIHSS score of 21 on admission. This patient was treated with intravenous recombinant tissue plaminogen activator (rtPA) only, and had an mRS score of 2 at 1 month follow-up.
Discussion
The BASICS study shows that patients ≥75 years with BAO have an increased risk of poor functional outcome and death compared with younger patients, despite comparable recanalization rates. In contrast with a small previous study [6], our data show that a substantial group of patients ≥75 years survives with good functional outcome.
Previously, it has been suggested that the increased risk of poor functional outcome in elderly patients resulted from a higher prevalence of atherosclerotic occlusions and consequently lower recanalization rates [3]. However, in our study population patients ≥75 years were more likely to have an embolic rather than an atherosclerotic cause of BAO, mainly due to a higher prevalence of atrial fibrillation. Patients ≥75 years with an embolic cause of BAO had a similar risk of poor functional outcome compared with patients in this age group with an atherosclerotic cause of BAO. Sufficient recanalization was achieved in 71 % of patients in this age group.
In patients ≥75 years, several baseline- and treatment-related characteristics were associated with an increased risk of poor functional outcome. A recent large case series of patients with BAO, in which only a minority of patients was ≥75 years, identified similar risk factors for poor functional outcome and death [7].
The strength of this study is that BASICS was a prospective registry of consecutive patients, and therefore our results are representative for daily practice. A limitation of this study is that this was a post hoc analysis of non-randomized data, and therefore the data regarding treatment-dependent outcomes are prone to bias. Due to the prospective collection of detailed data, we were able to perform Poisson regression analyses to adjust for important confounding baseline characteristics.
We conclude that a substantial group of elderly patients survives with a good functional outcome. This study cannot answer the question which treatment option is superior in elderly patients, nor can it define an upper age limit above which treatment is no longer effective. These and other questions may be answered in the recently started BASICS trial in which patients with BAO of up to 85 years of age are randomized between intravenous thrombolysis (IVT) alone vs. IVT followed by additional intra-arterial therapy (http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=2617; accessed February 1, 2012).
References
Hacke W, Zeumer H, Ferbert A, Brückmann H, del Zoppo GJ (1988) Intra-arterial thrombolytic therapy improves outcome in patients with acute vertebrobasilar occlusive disease. Stroke 19:1216–1222
Schonewille WJ, Wijman CA, Michel P, Rueckert CM, Weimar C, Mattle HP, Engelter ST, Tanne D, Muir KW, Molina CA, Thijs V, Audebert H, Pfefferkorn T, Szabo K, Lindsberg PJ, de Freitas G, Kappelle LJ, Algra A; on behalf of the BASICS study group (2009) Treatment and outcomes of acute basilar artery occlusion in the Basilar Artery International Cooperation Study (BASICS): a prospective registry study. Lancet Neurol 8:724–730
Brandt T, von Kummer R, Müller-Küppers M, Hacke W (1996) Thrombolytic therapy of acute basilar artery occlusion. Variables affecting recanalization and outcome. Stroke 27:875–881
Schonewille WJ, Algra A, Serena J, Molina CA, Kappelle LJ (2005) Outcome in patients with basilar artery occlusion treated conventionally. J Neurol Neurosurg Psychiatry 76:1238–1241
Goldmakher GV, Camargo EC, Furie KL, Singhal AB, Roccatagliata L, Halpern EF, Chou MJ, Biagini T, Smith WS, Harris GJ, Dillon WP, Gonzalez RG, Koroshetz WJ, Lev MH (2009) Hyperdense basilar artery sign on unenhanced CT predicts thrombus and outcome in acute posterior circulation stroke. Stroke 40:134–139
Ezaki Y, Tsutsumi K, Onizuka M, Kawakubo J, Yagi N, Shibayama A, Toba T, Koga H, Miyazaki H (2003) Retrospective analysis of neurological outcome after intra-arterial thrombolysis in basilar artery occlusion. Surg Neurol 60:423–429
Sairanen T, Strbian D, Soinne L, Silvennoinen H, Salonen O, Artto V, Koskela I, Häppölä O, Kaste M, Lindsberg PJ; Helsinki Stroke Thrombolysis Registry (HSTR) Group (2011) Intravenous thrombolysis of basilar artery occlusion: predictors of recanalization and outcome. Stroke 42:2175–2179
Nagel S, Schellinger PD, Hartmann M, Juettler E, Huttner HB, Ringleb P, Schwab S, Köhrmann M (2009) Therapy of acute basilar artery occlusion: intraarterial thrombolysis alone vs bridging therapy. Stroke 40:140–146
Schonewille WJ, Wijman CAC, Michel P, Algra A, Kappelle LJ, on behalf of the BASICS study group (2007) The Basilar Artery International Cooperation Study (BASICS). Int J Stroke 2:220–223
Greenland S, Finkle WD (1995) A critical look at methods for handling missing covariates in epidemiologic regression analyses. Am J Epidemiol 142:1255–1264
Acknowledgments
Development of the BASICS database was supported by the Department of Neurology, University Medical Centre Utrecht, The Netherlands.
Conflicts of interest
All authors report no disclosures.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
On behalf of the BASICS Study Group.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Vergouwen, M.D.I., Compter, A., Tanne, D. et al. Outcomes of basilar artery occlusion in patients aged 75 years or older in the Basilar Artery International Cooperation Study. J Neurol 259, 2341–2346 (2012). https://doi.org/10.1007/s00415-012-6498-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-012-6498-2