
Abstract
Background
The ability to predict the future progression of MS represents a key issue for the neurologist. The aim of the study was to create a multifactorial prognostic index (MPI) providing the probability of a severe MS course at diagnosis based on clinical and immunological CSF parameters.
Methods
64 clinically definite relapsing-remitting (RR)MS patients (38 benign, 26 severe MS) followed up for at least 10 years were included. Clinical and demographic details, EDSS after 5 and 10 years, progression index, relapse number and rate, time to a second relapse were assessed. CSF and serum samples collected at diagnosis were examined for CSF IgM and IgG oligoclonal bands (OB) and quantitative IgM and IgG determination.
Results
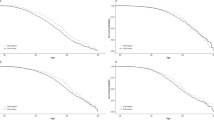
Kaplan-Meier analysis showed that the probability of reaching an EDSS score of 3 or 4 was significantly influenced by the presence of IgMOB (p < 0.01 and p < 0.01, log-rank test) and by the symptoms at onset (p = 0.04 and p = 0.03, log-rank test). These results were confirmed at multivariate analysis (Cox model). Univariate logistic analysis showed that IgMOB presence predicted a severe MS course (OR = 9.33, CI = 2.92– 29.88), whereas sensory symptoms at onset predicted a benign MS course (OR = 0.12, CI = 0.02–0.56). Using multivariate logistic regression the factors found to be significant were: presence/absence of IgMOB (p < 0.01), onset with sensory (p < 0.01) and pyramidal symptoms (p = 0.01), and first inter-attack interval (p = 0.03). The individual probability of a severe evolution was thus estimated by a simple formula comprising clinical and biological markers of prognosis available at diagnosis (pyramidal and sensory symptoms, months to the 2nd episode, and IgMOB presence/absence), giving the probability of developing a severe MS course. Applied to the same patient cohort this formula showed a global error of 6/64 (9.37 %). We then used another independent series of 65 RRMS patients to validate this model. In this second patient cohort, 4/45 BMS and 4/20 SMS patients were found to have been incorrectly classified (based on the formula), with a global error of 8/65 (12.31 %).
Conclusion
For the first time we created a MPI, using clinical and biological markers to predict the clinical course of MS at diagnosis. This index can support the clinician in patient counselling, therapeutic choices, as well as in patient selection criteria for clinical trials.
Similar content being viewed by others

References
Jacobs LD, Beck RW, Simon JH, Kinkel RP, Brownscheidle CM, Murray TJ, Simonian NA, Slasor PJ, Sandrock AW (2000) Intramuscular interferon beta-1a therapy initiated during a first demyelinating event in multiple sclerosis. CHAMPS Study Group. N Engl J Med 343:898–904
Comi G, Filippi M, Barkhof F, Durelli L, Edan G, Fernandez O, Hartung H, Seeldrayers P, Sorensen PS, Rovaris M, Martinelli V, Hommes OR; Early Treatment of Multiple Sclerosis Study Group (2001) Effect of early interferon treatment on conversion to definite multiple sclerosis: a randomised study. Lancet 357:1576–1582
Kuhlmann T, Lingfeld G, Bitsch A, Schuchardt J, Bruck W (2002) Acute axonal damage in multiple sclerosis is most extensive in early disease stages and decreases over time. Brain 125:2202–2212
Montalban X (2004) The pros and cons of early treatment of relapsing forms of multiple sclerosis. J Neurol 251 (Suppl 4):IV30–IV34
Confavreux C, Aimard G, Devic M (1980) Course and prognosis of multiple sclerosis assessed by the computerised data processing of 349 patients. Brain 103:281–300
Weinshenker BG, Rice GPA, Noseworthy J, Carriere W, Baskerville J, Ebers GC (1991) The natural history of multiple sclerosis: a geographically based study, 3. Multivariate analysis of predictive factors and models of outcome. Brain 114:1045–1056
Runmarker B, Andersen O (1993) Prognostic factors in a multiple sclerosis incidence cohort with 25 years of follow-up. Brain 116:117–134
Pittock SJ, McClelland RL, Mayr WT, Jorgensen NW, Weinshenker BG, Noseworthy J, Rodriguez M (2004) Clinical implications of benign multiple sclerosis: a 20-year population-based follow-up study. Ann Neurol 56:303–306
Uccelli A, Pedemonte E, Narciso E, Mancardi G (2003) Biological markers of the inflammatory phase of multiple sclerosis. Neurol Sci 24:S271–S274
Villar LM, Masjuan J, Gonzalez-Porque P, Plaza J, Sadaba MC, Roldan E, Bootello A, Alvarez-Cermeno JC (2002) Intrathecal IgM synthesis predicts the onset of new relapses and a worse disease course in multiple sclerosis. Neurology 59:555–559
Villar LM, Masjuan J, Gonzalez-Porque P, Plaza J, Sadaba MC, Roldan E, Bootello A, Alvarez-Cermeno JC (2002) Intrathecal IgM synthesis in neurological diseases. Relationship with disability in multiple sclerosis. Neurology 58:824–826
Villar LM, Masjuan J, Gonzalez-Porque P, Plaza J, Sadaba MC, Roldan E, Bootello A, Alvarez-Cermeno JC (2003) Intrathecal IgM synthesis is a prognostic factor in multiple sclerosis. Ann Neurol 53:222–226
Perini P, Ranzato F, Calabrese M, Battistin L, Gallo P (2006) Intrathecal IgM production at clinical onset correlates with a more severe disease course in Multiple Sclerosis. J Neurol Neurosurg Psychiatry 77:953–955
Kurtzke JF, Beebe GW, Nagler B, Kurland LT, Auth TL (1977) Studies on the natural history of multiple sclerosis-8. Early prognostic features of the later course of the illness. J Chronic Dis 30:819–830
Kurtzke JF (1983) Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33:1444–1452
Villar LM, Gonzales-Porquè P, Masjuan J, Alvarez-Cormeno JC, Bootello A, Keir G (2001) A sensitive and reproducible method for the detection of oligoclonal IgM bands. J Immunol Methods 258:151–155
Sharief MK, Thompson EJ (1991) Intrathecal immunoglobulin M synthesis in multiple sclerosis. Relationship with clinical and cerebrospinal fluid parameters. Brain 114:181–195
Roxburgh RH, Seaman SR, Masterman T, Hensiek AE, Sawcer SJ, Vukusic S, Achiti I, Confavreux C, Coustans M, le Page E, Edan G, McDonnell GV, Hawkins S, Trojano M, Liguori M, Cocco E, Marrosu MG, Tesser F, Leone MA, Weber A, Zipp F, Miterski B, Epplen JT, Oturai A, Sorensen PS, Celius EG, Lara NT, Montalban X, Villoslada P, Silva AM, Marta M, Leite I, Dubois B, Rubio J, Butzkueven H, Kilpatrick T, Mycko MP, Selmaj KW, Rio ME, Sa M, Salemi G, Savettieri G, Hillert J, Compston DA (2005) Multiple Sclerosis Severity Score: using disability and disease duration to rate disease severity. Neurology 64:1144–1151
Amato MP, Ponziani G (2000) A prospective study on the prognosis of multiple sclerosis. Neurol Sci 21:S831–S838
Avasarala JR, Cross AH, Trotter JL (2001) Oligoclonal band number as a marker for prognosis in multiple sclerosis. Arch Neurol 58:2044–20 45
Bergamaschi R, Berzuini C, Romani A, Cosi V (2001) Predicting secondary progression in relapsing-remitting multiple sclerosis: a Bayesian analysis. J Neurol Sci 189:13–21
Tintoré M, Rovira A, Rio J, Nos C, Grivé E, Téllez N, Pelayo R, Comabella M, Montalban X (2005) Is optic neuritis more benign than other first attacks in multiple sclerosis? Ann Neurol 57:210–215
Sharief MK, Keir G, Thompson EJ (1990) Intrathecal synthesis of IgM in neurological diseases: a comparison between detection of oligoclonal bands and quantitative estimation. J Neurol Sci 96:131–142
Sindic CJM, Monteyne P, Laterre EC (1994) Occurrence of oligoclonal IgM bands in the cerebrospinal fluid of neurological patients: an immunoaffinity-mediated capillary blot study. J Neurol Sci 124:215–219
Lolli F, Siracusa G, Amato MP, Fratiglioni L, Dal Pozzo G, Galli E, Amaducci L (1991) Intrathecal synthesis of free immunoglobulin light chains and IgM in initial multiple sclerosis. Acta Neurol Scand 83:239–243
Walsh MJ, Tourtellotte WW (1986) Temporal invariance and clonal uniformity of brain and cerebrospinal IgG, IgA and IgM in multiple sclerosis. J Exp Med 163:41–53
Correale J and de los Milagros Bassani Molinas M (2002) Oligoclonal bands and antibody responses in Multiple Sclerosis. J Neurol 249:375–389
Sellebjerg F, Christiansen M, Garred P (1998) MBP, anti-MBP and anti-PLP antibodies, and intrathecal complement activation in multiple sclerosis. Mult Scler 4:127–131
Mead RJ, Singhrao SK, Neal JW, Lassmann H, Morgan BP (2002) The membrane attack complex of complement causes severe demyelination associated with acute axonal injury. J Immunol 168:458–465
Lucchinetti CF, Mandler RN, McGavern D, Bruck W, Gleich G, Ransohoff RM, Trebst C, Weinshenker B, Wingerchuk D, Parisi JE, Lassmann H (2002) A role for humoral mechanisms in the pathogenesis of Devic’s neuromyelitis optica. Brain 125:1450–1461
Villar LM, Sadaba MC, Roldan E, Masjuan J, Gonzalez-Porque P, Villarrubia N, Espino M, Garcia-Trujillo JA, Bootello A, Alvarez-Cermeno JC (2005) Intrathecal synthesis of oligoclonal IgM against myelin lipids predicts an aggressive disease course in MS. J Clin Invest 115:187–194
O’Riordan JI, Thompson AJ, Kingsley DP, MacManus DG, Kendall BE, Rudge P, McDonald WI, Miller DH (1998) The prognostic value of brain MRI in clinically isolated syndromes of the CNS. A 10-year follow-up. Brain 121:495–503
Pittock SJ, Mayr WT, McClelland RL, Jorgensen NW, Weigand SD, Noseworthy JH, Rodriguez M (2004) Disability profile of MS did not change over 10 years in a population-based prevalence cohort. Neurology 62:601–606
Tremlett H, Paty D, Devonshire V (2006) Disability progression in multiple sclerosis is slower than previously reported. Neurology 66:172–177
Pittock SJ (2006) Therapeutic decision making in MS: impact of a slower disability progression. Neurology 66:157
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mandrioli, J., Sola, P., Bedin, R. et al. A multifactorial prognostic index in multiple sclerosis. J Neurol 255, 1023–1031 (2008). https://doi.org/10.1007/s00415-008-0827-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-008-0827-5