
Abstract
Purpose
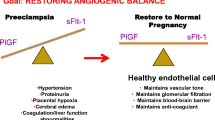
The aim of our study was to elucidate the role of IPF in preeclampsia, because the immature platelet fraction (IPF) is available in most emergency departments. A number of parameters have been introduced to diagnose preeclampsia/HELLP syndrome. The defined cutoffs of angiogenic and antiangiogenic parameters, soluble fms-like tyrosine kinase 1 and placental growth factor, have been approved for clinical routine. However, these parameters need complex analysis and are expensive.
Methods
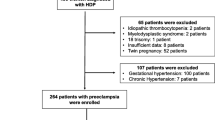
The data of 69 pregnant women between 20 and 42 weeks of gestation were analyzed in this retrospective monocentric study. 28 of them had preeclampsia, HELLP syndrome or partial HELLP syndrome fitting the Tennessee criteria (study group 1). Furthermore, 41 normotensive pregnant women were included as controls (study group 2). In both groups the IPF was analyzed.
Results
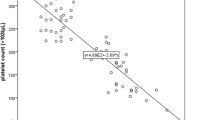
In this study, we demonstrated that the values of IPF were significantly higher in patients with hypertensive diseases than in normotensives, but could not distinguish between preeclampsia and HELLP syndrome. The absolute number of immature platelets of women with preeclampsia was significantly higher and those of HELLP syndrome were significantly lower than values of healthy women. The absolute number of immature platelets as well as mature thrombocytes helps to distinguish between HELLP syndrome and preeclampsia.
Conclusion
IPF levels are higher in women with hypertensive pregnancy than in normotensive controls. They could be used to diagnose hypertensive diseases in pregnancy. To distinguish between preeclampsia and HELLP syndrome, thrombocytes or the absolute number of immature platelets is needed.



Similar content being viewed by others
References
Magee LA, Abalos E, von Dadelszen P, Sibai B, Easterling T, Walkonshaw S (2011) How to manage hypertension in pregnancy effectively. Br J Clin Pharmacol 72:394–401
Moussa HN, Arian SE, Sibai BM (2014) Management of hypertensive disorders in pregnancy. Women’s Health 10:385–404
Milne F, Redman C, Walker J, Baker P, Bradley J, Cooper C et al (2005) The pre-eclampsia community guideline (PRECOG): how to screen for and detect onset of pre-eclampsia in the community. Br Med J 330:576–580
Duley L (2009) The global impact of pre-eclampsia and eclampsia. Semin Perinatol 33:130–137
Sibai BM (1990) The HELLP syndrome (hemolysis, elevated liver enzymes, and low platelets): much ado about nothing? Am J Obstet Gynecol 162:311–316
Maged AM, Saad H, Meshaal H, Salah E, Abdelaziz S, Omran E, Deeb WS, Katta M (2017) Maternal serum homocysteine and uterine artery Doppler as predictors of preeclampsia and poor placentation. Arch Gynecol Obstet 296(3):475–482. https://doi.org/10.1007/s00404-017-4457-y
Stepan H, Jank A (2009) Angiogene Faktoren und ihre Rolle in der Entstehung und Vorhersage der Präeklampsie. ZNG 213:101–105
Verlohren S, Herraiz I, Lapaire O, Schlembach D, Moertl M, Zeisler H et al (2012) The sFlt-1/PlGF ratio in different types of hypertensive pregnancy disorders and its prognostic potential in preeclamptic patients. Am J Obstet Gynecol 206(58):e1–e8
Verlohren S, Herraiz I, Lapaire O, Schlembach D, Zeisler H et al (2014) New gestational phase-specific cutoff values for the use of the soluble fms-like tyrosine kinase-1/placental growth factor ratio as a diagnostic test for preeclampsia. Hypertension 63:346–352
Kose S, Tuna G, Nuriyeva G, Altunyurt S, Islekel GH, Doğan OE (2018) A prospective cohort study on the prediction of the diagnosis-to-delivery time in preeclamptic pregnancies: should the sFlt-1/PlGF ratio be added to routine evaluations? Arch Gynecol Obstet 298(5):911–920. https://doi.org/10.1007/s00404-018-4903-5
Verlohren S, Stepan H, Dechend R (2012) Angiogenic growth factors in the diagnosis and prediction of preeclampsia. Clin Sci 122:43–52
Everett TR, Garner SF, Lees CC, Goodall AH (2014) Immature platelet fraction analysis demonstrates a difference in thrombopoiesis between normotensive and preeclamptic pregnancies. J Thromb Haemost 111:1177–1179
Rinder HM, Bonan JL, Anandan S, Rinder CS, Rodrigues PA et al (1994) Noninvasive measurement of platelet kinetics in normal and hypertensive pregnancies. Am J Obstet Gynecol 170:117–122
Kazmi R, Cooper A, Lwaleed B (2011) Platelet function in pre-eclampsia. Semin Thromb Hemost 37:131–136
Ratsch U, Kaiser T, Stepan H, Jank A (2017) Evaluation of bone marrow function with immature platelet fraction in normal pregnancy. Hypertens Pregnancy 10:70–73
Moraes D, Munhoz PT, Pinheiro da Costa BE, Hentschke MR, Sontag F, Silveira Lucas L et al (2016) Immature platelet fraction in hypertensive pregnancy. Platelets 27:333–337
Author information
Authors and Affiliations
Contributions
UB: protocol/project development, data collection, data analysis, manuscript writing/editing. TK: data collection or management. HS: manuscript writing/editing. AJ: protocol/project development, data analysis, manuscript writing/editing/correcting and adding the revisions.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest relevant to this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bernstein, U., Kaiser, T., Stepan, H. et al. The immature platelet fraction in hypertensive disease during pregnancy. Arch Gynecol Obstet 299, 1537–1543 (2019). https://doi.org/10.1007/s00404-019-05102-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-019-05102-2