
Abstract
Case report
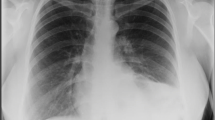
We report on a 30-year old woman presenting with symptoms of hyperemesis gravidarum and subsequent vomiting at the end of the first trimester (12 + 0 weeks of gestation). The patient was initially presented with nausea and vomiting, without any signs or symptoms of intra-abdominal disorders. On the 2nd day, symptoms became worse and she complained right sided upper abdominal pain, therefore abdominal ultrasound was performed, showing no remarkable findings, explaining the disorder. Clinical symptoms increased and the patient complained suddenly severe dyspnoea and intractable cough. Therefore, immediately an X-ray examination of the thorax was performed showing a severe left sided diaphragmatic hiatus hernia with consecutive displaced stomach into the thoracic cavity, making immediate surgical intervention necessary.
Discussion
Diaphragmatic hernias complicating pregnancy are a rare event, they normally occur in later periods of pregnancy due to the rising intra-abdominal pressure mainly caused by the enlargement of the uterus. Also maternal diaphragmatic hernias during pregnancy are usually associated with minor complains. However, they can be life-threatening, due to mediastinal shift and cardio-respiratory failure. The majority of maternal diaphragmatic hernias complicating pregnancies occur in antenatal period, most of them in the third trimester. More than 90% of maternal diaphragmatic hernias complicating pregnancy are localized on the left side of the maternal diaphragma. We present a case of an early onset life-threatening maternal diaphragmatic hernia. Usually, maternal diaphragmatic hernias become clinically obvious in advanced stage of pregnancy, in contrast hyperemesis gravidarum is normally occurring in the first trimester and is usually self-limiting. Guiding symptoms for hyperemesis gravidarum are nausea and vomiting, but these clinical findings can also be unspecific symptoms of a maternal diaphragmatic hernia. Therefore, especially mild variants of maternal diaphragmatic hernias in early pregnancy can be misdiagnosed as hyperemesis gravidarum. Nevertheless, the rising intra-abdominal pressure while vomiting obviously can trigger exacerbation of a pre-existing maternal diaphragmatic hernia. We therefore speculate that there could be an association between physiological changes in early pregnancy, for example in gastric motility, and the exacerbation of the pre-existing maternal hiatus hernia.
Conclusion
Hence a diaphragmatic hernia should always be excluded, if symptoms of nausea and vomiting are intractable, mediastinal shift with dyspnoea occurs, failure of conservative treatment especially after 20th week of gestation and in late onset of assumed hyperemesis gravidarum.


Similar content being viewed by others


References
Gadsby R, Barnic-Adshead AM, Jagger C (1993) A prospective study of nausea and vomiting during pregnancy. Br J Gen Pract 43:245–248
Kallen B (1987) Hyperemesis during pregnancy and delivery outcome: a registry study. Eur J Obstet Gynecol 26:291–302
Tsang IS, Katz VL, Wells SD (1996) Maternal and fetal outcomes in hyperemesis gravidarum. Int J Gynecol Obstet 55:231–235
Jordan V, MacDonald J, Crichton S, Ford H (1995) The incidence of hyperemesis gravidarum is increased among Pacific Islanders living in Wellington. NZ Med J 108:342–344
Fairweather DV (1968) Nausea and vomiting in pregnancy. Am J Obstet Gynecol 102:135–175
Flaxman SM, Sherman PW (2000) Morning sickness: a mechanism for protecting mother and embryo. Q Rev 75:113–148
Verberg MF, Gillot DJ, Al-Fardan N, Grudzinskas JG (2005) Hyperemesis gravidarum, a literature review. Hum Reprod Updat 11(5):527–529
Michelini GA (2002) Hyperemesis gravidarum. Emedicine 12(2)
Michel ME, Alanio E, Bois E, Gavillon N, Graesslin O (2010) Wernicke encephalopathy complicating hyperemesis gravidarum: a case report. Eur J Obstet Gynecol Reprod Biol 149(1):118–119
Valiulis B, Kelley RE, Hardjasudarma M, London S (2001) Magnetic resonance imaging detection of a lesion compatible with central pontine myelinolysis in pregnant patient with recurrent vomiting and confusion. J Neuroimaging 11(4):441–443
Kanayama N, Khatun S, Belayet HM, Yamashita M, Yonezawa M, Kobayashi T, Terao T (1998) Vasospasm of cerebral arteries in hyperemesis gravidarum. Gynecol Obstet Invest 46(2):139–141
Nel JT, Van Heyningen CF, Van Eeden SF, Labadarios D, Louw NS (1985) Thiamine deficiency-induced gestational polyneuropathy and encephalopathy a case report. S Afr Med J 67(15):600–603
Devignes J, Grare M, Raft J, Vial F, Hacquard M, Bouaziz H, Lecompte T, De Maistre E (2009) A case of cutaneous and mucous haemorrhage secondary to vitamin K deficiency in hyperemesis gravidarum. Ann Fr Anesth Reanim 28(7–8):697–700
Robinson JN, Banerjee R, Thiet MP (1998) Coagulopathy secondary to vitamin K deficiency in hyperemesis gravidarum. Obstet Gynecol 92(4 Pt2):673–675
Liang SG, Ooka F, Santo A, Kaibara M (2002) Pneumomediastinum following esophageal rupture associated with hyperemesis gravidarum. J Obste Gynecol Res 28:172–175
Joseph P, Raju RS, Vyas FL, Sitaram V (2008) Spontaneous perforation of choledochal cyst and hyperemesis gravidarum. Trop Gastroenterol 29(1):46–47
Ghani R (2003) The use of total parenteral nutrition in protracted hyperemesis gravidarum. J Obstet Gynecol 23:199–201
Mazotta P, Magee L, Koren G (1996) Therapeutic abortions due to severe morning sickness: an unacceptable combination. The Mothersick Newsletter 1–3
Jarnfelt-Samsioe A, Samsioe G, Velinder GM (1983) Nausea and vomiting in pregnancy—a contribution to its epidemiology. Gynecol Obstet Invest 16:221–229
Eglinton TW, Coulter GN, Bagshaw PF, Cross LA (2006) Diaphragmatic hernias complicating pregnancy. ANZ J Surg 76:553–557
Van den Hout L, Sluiter I, Gischler S, De Klein A, Rottier R, Ijsselstijn H, Reissl I, Tibboel D (2009) Can we improve outcome of congenital diaphragmatic hernia? Pediatr Surg Int 25(9):733–743
De Buys Roessingh AS, Dinh-Xuan AT (2009) Congenital diaphragmatic hernia: current status and review of the literature. Eur J Pediatr 168(4):393–406
Babel N, Sakpal SV, Shah S, Feldman S, Chamberlain RS (2009) Chronic diaphragmatic hernia: a delayed problem requiring urgent response. ANZ J Surg 79(10):754–755
Jawad AJ, Al-Samarrai AL, Al-Mofada S, Al Howasi M, Hawass NE, Al-Beiruti Z (1998) Congenital para-oesophageal hiatal hernia in infancy. Pediatr Surg Int 13(2–3):91–94
Larusson HJ, Zingg U, Hahnloser D, Delport K, Seifert B, Oertli D (2009) Predictive factors for morbidity and mortality in patients undergoing laparoscopic paraesophageal hernia repair: age, ASA score and operation type influence morbidity. World J Surg 33(5):980–985
Osmak L, Cougard P (2003) Diaphragmatic hernia. Rev Prat 53(15):1683–1687
Ting JY (2008) Difficult diagnosis in the emergency department: hyperemesis in early trimester pregnancy because of incarcerated maternal diaphragmatic hernia. Emerg Med Australas 20:441–443
Yang X, Liu R, Dong Y (2006) Regulative effects of ovarian steroids on rat gastric motility and sensitivity. Acta Physiol 58(3):275–280
Sase M, Lee JJ, Ross MG, Buchmiller TL (2005) Maternal steroid enhancement of fetal rabbit gastrointestinal motility. J Obstet Gynecol Res 31(3):263–267
Kusama T, Ota K (2002) Radiological protection for diagnostic examination of pregnant women. Congenit Anom 42(1):10–14
Osei EK, Faulkner K (1999) Fetal doses from radiological examinations. Br J Radiol 72:773–778
Conflict of interest
All authors declare no conflict of interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schwentner, L., Wulff, C., Kreienberg, R. et al. Exacerbation of a maternal hiatus hernia in early pregnancy presenting with symptoms of hyperemesis gravidarum: case report and review of the literature. Arch Gynecol Obstet 283, 409–414 (2011). https://doi.org/10.1007/s00404-010-1719-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-010-1719-3