
Abstract
Purpose
We aimed to investigate whether parental and siblings’ sugar-sweetened beverage (SSB) intake had prospective impact on children’s SSB consumption, and the potential sex difference in these associations.
Methods
This study included a total of 904 children and their parents enrolled from 2004 to 2011 China Health and Nutrition Survey (CHNS) cohort study. SSB consumption information was estimated using a short dietary questionnaire and total energy intake was assessed with three-day 24-h dietary assessments at recruitment and follow-up surveys. Multivariate logistic or linear regression analyses were used to assess the association for SSB consumption between parents, siblings and children after adjusting for age, body mass index (BMI) z-score, household income and parental educational level.
Results
In this study, a majority (87.6%) of children consumed SSB. Among them, the median consumption of SSB was 70.3 ml/day per capita and 205.4 ml/day per consumer. Parental SSB consumption was relevant to children’s SSB consumption, and this association was more pronounced in boys than in girls. Meanwhile, fathers seemed to have a stronger impact on whether children consume SSB than mothers which was reflected by lower P and higher OR. Additionally, children’s SSB intake was prospectively associated with their older siblings’ SSB consumption (P for trend < 0.03).
Conclusions
Parental and older siblings’ SSB consumption was relevant to children’s SSB intake. Particularly, boys were more susceptible to parental impact than girls, and fathers seemed to have a greater influence on children than mothers.
Similar content being viewed by others

Introduction
Over the last 20 years, epidemiological studies have indicated a 24.4% increment of sugar-sweetened beverage (SSB) consumption among Chinese children [1]. Higher SSB consumption is an established risk factor for childhood obesity and dental caries [2] and is suggested to be associated with cancer [3], cardiovascular disease and metabolic syndrome later in life [4]. Thus, to protect children from health problems and health hazards, more attention is required to address the causes and factors influencing children’s SSB consumption.
Family factors have been proved to be one of the main influencing factors affecting children’s SSB consumption, and associations between family members’ SSB consumption and children’s diet with high SSB intake have been found in cross-sectional studies [1, 5,6,7,8,9,10,11,12,13]. While the correlation is strong, it is not possible to unequivocally determine the direction of causality. A bidirectional relationship may exist between adolescents and family members [14]. Thus, prospective studies with a clearly defined temporal relationship are more convincing than cross-sectional studies in elucidating potentially causal links between family members’ SSB consumption and children’s SSB intake. Moreover, sex differences in intergenerational relationships between parents and offspring were found in alcohol consumption [15] and physical activity [16], and sex difference also exists in SSB drinking behavior [17]. These lead us to speculate on the possible sex differences in the association for SSB intake between parents and children, which did not attract widespread attention yet.
Among family members, an important area of study is the extent to which the SSB consumption patterns of adults influence those of children in their households. Most studies that describe SSB consumption within families assess one child with one parent [5, 6, 8, 10,11,12] or guardian [7, 9]. It is argued that fathers and mothers provided different experiences for adolescents’ health status [18]. Only conducted in one parent may induce selection bias. In addition to parents, siblings could be another influencing factor for children to establish health attitudes toward physical activity[19] and dietary habits [20], such as eating frequency and food diversity. To date, there is only one cross-sectional study in Great Britain that indicated the role of siblings on children’s SSB consumption [13]. And this association, to our knowledge, has never been explored thus far in China.
Considering the secular trend of increasing SSB intake in Chinese children and its short- and long-term health concerns, this study aimed to investigate whether family members’ SSB consumption was prospectively associated with children’s SSB intake, including: (1) parental impact on children’s SSB consumption, and potential sex difference; (2) sibling’s impact on children’s SSB intake.
Subjects and methods
China health and nutrition survey
China health and nutrition survey (CHNS), an ongoing household-based open cohort, has been conducted 11 waves in 15 provinces and municipal cities in China between 1989 and 2015. In brief, CHNS uses a multistage random cluster sampling method to select a demographically representative Chinese sample. All participants provided written informed consent in the survey [21] and could join or withdraw from the study at any survey wave. The study protocol was approved by the ethical review committees of the Chinese Center for Disease Control and Prevention and the University of North Carolina at Chapel Hill. Detailed description of CHNS design can be found on its official website [22].
Study sample
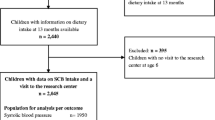
Data obtained from the China Health and Nutrition Survey are publicly available [23]. Since information on SSB consumption was collected in 2004, 2006, 2009 and 2011, the present analysis is based on these four waves of the survey. By the end of 2011, a total of 2620 offspring–father–mother trios provided data on SSB intake. Among them, offspring–father–mother trios (1) with offspring’s age was above 18 years old or less than 6 years (n = 392), or (2) with one wave of SSB data (n = 1324) were excluded. There were only small differences in the general characteristics of the included and excluded subjects (Table S1). In total, 904 child–father–mother trios were included in the analysis of the association for SSB consumption between parents and children, and 265 child–sibling dyads were included in the analysis of the association between siblings and children (Fig. 1a). A post-hoc power test (SAS proc power procedure) showed that the power was > 0.999 for the parental impact on children’s SSB consumption, and 0.776 for the sibling’s impact on children’s intake. The values were comparable to the criteria (0.8) introduced by Cohen [24]. To assure the exact chronological order of data collection, SSB data of children were collected in 2006, 2009 and 2011, and SSB data of parents and siblings were traced back 2–5 years for children’s SSB data (Fig. 1b). If parents or siblings had multiple waves of SSB consumption data, only data from the wave closest to the wave of children’s SSB data were retained.

Data selection of study sample. a Flowchart for the selection of the analyzed study sample. b Chronological order of data collection from children to parents and siblings. SSB data of children were collected in 2006, 2009 and 2011, and SSB data of parents and siblings were traced back 2–5 years from children’s SSB data. And if parents or siblings had multiple waves of SSB consumption data, only data from the wave closest to the wave of children’s SSB data were retained
Dietary assessment
SSB consumption data were collected by trained personnel in personal interviews using a short dietary questionnaire from a structured individual questionnaire [25]. Children aged 6–10 years provided information with the help of parents or guardians, and others provided information on their own. SSB intake was obtained by these questions, ‘In the last year, did you drink SSB, and how much SSB did you drink each week?’. According to CHNS procedure, SSB was defined as Coca-Cola, soda, lemonade and juices with no more than 10% pure fruit juices [26].
Since complete dietary information is unavailable in the short dietary questionnaire, data on total energy intake was obtained from valid three consecutive 24-h recalls [27]. According to CHNS regulations, parents and children aged 12 years and older were asked to recall all foods and beverages they consumed. For children below 12 years, their parents or guardians provided information on food consumption at home, while children provided information on dietary intake away from home. The majority of participants (99.7%) completed three-day 24-h recalls (i.e., 42.4% had three weekdays, 29.0% had two weekdays and one weekend day, 18.7% had one weekday and two weekend days, and 9.6% had three weekend days) and only 3 children (0.3%) finished two-day 24-h recalls (i.e., 2 children had two weekdays, and 1 child had one weekday and one weekend day).
Socio-demographic characteristics
Detailed information on socio-demographic characteristics was collected using a structured questionnaire at baseline, including sex, age (continuous variable), residency (urban and rural), education of father or mother (< 6 years, 6–12 years, > 12 years of schooling) and household monthly personal income (≤ 1800 CNY (Chinese Yuan), 1800–3200 CNY, ≥ 3200 CNY) [28].
Children aged 6–17 years were classified either as single child or child with sibling(s) after checking the matched household ID and parent ID in the CHNS dataset.
Anthropometric measurements for children were measured by the trained investigators following standard procedures [29]. Height was measured to the nearest 0.1 cm using a tape measure (Mechanical Measuring Tape No. 206; SECA) without shoes, and weight was measured to the nearest 0.1 kg using a weight scale (Floor Weight Scale No. 877; SECA, UK) with lightweight clothing [30]. In this analysis, body mass index (BMI) was calculated as weight divided by height squared (kg/m2). Age-specific BMI z-scores were calculated based on the Chinese children’s reference curves [31].
Statistical analysis
Statistical Analyses System procedures (SAS, version 9.3, 2011, NC, USA) were used for all data analyses. Missing values (< 3%) of socio-demographic characteristics were substituted by mean and mode to substitute in the continuous and categorical variables, respectively [32]. A P-value < 0.05 was considered statistically significant, except for the interaction, where P-value < 0.1 was considered significant.
For categorical variables (sibship, income, residency and SSB consumption), frequencies were calculated. For continuous variables, BMI z-score was presented as means and standard deviation due to normal distributions; age and amounts of SSB consumption for consumers were presented as median and quartiles due to non-normal distributions. To obtain more information about the variation, the amount of SSB consumption for all participants was presented as mean (fifth percentile, ninety-fifth percentile) [33]. Differences in absolute amounts of SSB consumption, age, anthropometric data, sibship, income and residency between boys and girls were tested by Chi-square test for categorical variables, Student’s t-test for normally distributed continuous variables, and Kruskal–Wallis test for non-normally distributed continuous variables. Differences in the proportion of SSB consumers between the only-child and those with sibling(s), grouped by sex and parental SSB consumption, were tested by Fisher’s exact test.
To investigate the relevance of paternal, maternal or parental SSB consumption with offspring’s SSB intake (consume or not) across sex, multivariable logistic regression models were used. Parental SSB consumption was divided into three groups: (1) neither consumes (father and mother both do not drink SSB); (2) only one consumes (father or mother drink SSB); and (3) both consume (father and mother both drink SSB). In the basic models, paternal/maternal/parental SSB consumption were an independent predictor, respectively. In the adjusted model, variables potentially affecting this relevance were considered: age of offspring, BMI z-score, household monthly personal income, residency, sibship, age of parent, and parental educational level. In sensitive analysis, to test the robustness of our results, we repeated the logistic analysis within the participants without missing values on socio-demographic characteristics.
Among dyads with parents and children both consuming SSB, the relevance of parental amount of SSB intake on children’s amount of SSB consumption was tested using multivariable linear regression. Energy-adjusted (nutrient residual) model was used to adjust parents’ and children’s SSB consumptions [34]. The adjusted models were constructed in analogy to the multivariable logistic regression analyses. Multicollinearity was not found between independent variables and the socio-demographic characteristics (variance inflation factors < 3).
To investigate the prospective associations for SSB intake (consume or not) between siblings and children, multivariable logistic regression models were used. First, in the basic model, elder siblings’ SSB intake was regarded as an independent predictor. The sex of the younger child, the age difference between the two children in a household, and parental SSB consumption were considered as potentially affecting variables in the adjusted model. Second, younger siblings’ SSB intake was considered as an independent predictor in the basic model. This relevance was examined with the adjustment for the sex of elder children, the age difference between two children in a household, and parental SSB consumption in the adjusted model.
Results
Participant characteristics
The characteristics of 904 children are presented in Table 1. At the baseline, children had a median age of 12 (9, 14), and a mean BMI z-score of − 0.4 ± 1.2. There were slightly more boys (53.3%) than girls in this study. Most of the participants were only child and more than 85% of the participants were SSB consumers. Compared to children, a lower proportion of parents were SSB consumers and they also had a lower absolute amount of SSB intake. Among all participants, the mean intake of SSB was 70.3 ml/day for children, 23.2 ml/day for fathers and 19.7 ml/day for mothers. Among SSB consumers, the median intake of SSB was 205.4 ml/day for children, 35.7 ml/day for fathers and 21.4 ml/day for mothers.
Association for SSB consumption between parents and children
The multivariable logistic analysis for the prospective associations for SSB intake between parents and offspring is presented in Table 2. In boys and girls, the chance of being an SSB consumer was significantly higher if their parents were SSB consumers.
For the difference between boys and girls, we found that odd ratios (ORs) for the association between boys’ SSB consumption and paternal/maternal SSB intake were 0.3–0.7 times higher than the ORs for the association between girls’ SSB consumption and parental/maternal SSB intake (paternal consumption: OR for boys = 5.4 vs. OR for girls = 3.2; maternal intake: OR for boys = 2.5 vs. OR for girls = 2.0). And for the difference between fathers and mothers, we found that the OR of fathers was 1.2 times higher than that of mothers among boys (OR for fathers = 5.4 vs. OR for mothers = 2.5) and 0.6 times higher among girls (OR for fathers = 3.2 vs. OR for mothers = 2.0).
Furthermore, compared with boys whose neither fathers nor mothers consumed SSB, boys with one parent drinking SSBs had a 2.5 times higher chance of consuming SSB, and a 5.3 times higher chance if two parents were SSB consumers. Compared with girls whose neither fathers nor mothers consumed SSB, the chance of consuming SSB was not different among girls with one parent drinking SSB, and the chance was 4.7 times higher among girls with two parents drinking SSB.
Sensitivity analyses showed no substantial changes in the results after excluding participants with missing values for the socio-demographic characteristics (Table S2). Similar results were also found in the association for amount of SSB consumption between parents and children (Table S3).
Association for SSB consumption between siblings and children
Moreover, when parental SSB consumption was in the same condition, children who have sibling(s) were less likely to consume SSB than those without siblings (Figure S1; Table S4). There was an interaction between sibship and the associations of parental SSB intake with children’s SSB consumption (P for interaction = 0.05). The impact of siblings’ SSB intake on children’s SSB consumption is presented in Table 3. The adjusted logistic regression model showed that the chance of being an SSB consumer increased if the elder sibling was an SSB consumer (OR = 4.9, 95% CI, 1.1–21.1). However, younger siblings’ SSB intake was not statistically relevant to children’s SSB consumption (P for trend > 0.06).
Discussion
In the present study, higher parental SSB consumption was prospectively associated with higher children’s SSB intake, and this association was more pronounced in boys than in girls, and fathers had a stronger impact than mothers. Additionally, children’s SSB consumption was influenced prospectively by their older siblings’ SSB intake rather than younger siblings’.
In the present study, children with parents who drink SSB were more likely to consume SSB, which was in line with the studies in 2–17 years old children and adolescents from the US [6, 9, 12], and 8–12 years old children from New Zealand [8]. Parents serve as role models for children’s behavior [5], and parental intake of vegetables and fruit, red meat, dairy and dairy products can directly affect children’s consumption of these foods and beverages [35, 36]. In addition, foods are mainly prepared and purchased by parents at home [37], and those with a diet rich in SSB might often store SSBs at home and may be less apt to restrict or have rules on their children’s SSB consumption. The availability and consumption of SSB for these children would, thus, be higher than those with parents who seldom drink SSB. Other than parental dietary behavior, previous researchers examined parental educational levels were examined as a factor in children’s SSB consumption [38]. Higher-educated parents tended to be well-off economically [39]. In this study, 88.2% of parents were high school graduates or below and two-thirds of households have a monthly personal income of less than 3200 Yuan (488.7 $). When parents consume SSB, the odds of children consuming SSB were lower in this study (OR:5.3; 95%CI: 1.4, 14.2) than in the US study (OR:8.9; 95%CI:4.6, 17.3) with a higher parental education level and a good socioeconomic status [12]. This contradiction might be explained by different SSB market prices. In developing countries, SSBs were usually less affordable than in western countries [40], and Chinese parents of better economic status may be the ones who regularly buy SSBs for their children, while in the United States, low-income parents often choose to feed their children with low-priced SSB [8]. Additionally, this study included a relatively large number of rural children. Supermarkets are far from their places of residence, and these families may go to the supermarket once in a very long time to make purchases. Some rural areas in China are located in mountainous areas with inconvenient transportation[41], and parents living in these areas would buy more household necessities rather than expensive and heavy SSBs. These would decrease the accessibility of SSB to children. Different amounts of SSB intake may also have contributed to the difference. In our study, the median SSB consumption of Chinese children was 70.3 ml/day, which was much lower than the mean SSB consumption of children in the USA (419.2 ml/day) [32].
Potential sex differences were found in intergenerational relationships between parents and their offspring [15, 16]. In this analysis, we paid special attention to the sex differences and found that boys’ SSB consumption was more susceptible to their parents' SSB intake than girls’, and fathers seemed to have a greater influence on whether children consume SSB than mothers. These differences may be explained by different attitudes towards consuming SSB between males and females, and diverse parenting styles in sons and daughters. First, different attitudes have been shown to produce different patterns of behavior [42]. In adults, the prevalence of sweetened soft drink consumption for men was higher by at least 5% than for women [17]. In children, boys tend to link the behavior of consuming SSB, especially carbonated beverages, with “popular”, “cool”, and “risky”, and have a positive attitude toward SSB [43,44,45]. When they witness others drinking SSB, to make themselves look cool and popular, they are more inclined to choose SSB rather than plain water. Girls, however, tend to link the behavior of consuming healthy beverages with good body shape and are more inclined to choose plain water and 100% juice instead of SSB [44, 46, 47]. Secondly, different parenting styles would lead to different parent–child intimacy communication styles [48]. In China, authoritative parenting styles were often found in boys’ families [49]. Boys in these families are more likely to imitate their parents’ behavior to reduce the possibility of being scolded for making mistakes. When witnessing parents drinking SSB, to imitate their behavior, boys may choose SSB. Democratic styles were often found in girls’ families [49], they are less likely to drink SSB to imitate parental behavior.
In this study, fathers seemed to have a greater influence on whether children consume SSB than mothers, which was inconsistent with a recent cross-sectional study in Chinese population [1]. The studies were of the same population, and socio-demographic parameters were relatively similar. The discrepancy between studies may be related to the different methodologies and different selections of participants. Selection of study participants and detained processing of children with multiple surveys were unknown in that study, the same child could be included as a study participant more than once. In Chinese population, fathers instead of mothers were proved to have an impact on children’s dietary protein intake [50], implying that a similar role may exist in SSB consumption. This hypothesis requires further investigation in longitudinal studies. While we do find that boys were 1.3–1.7 times more likely to be influenced by their parental SSB consumption than girls, the bias due to inevitable limitations challenges the validity of these findings, including observational nature of the study, selection bias, missing data and measurement error. However, this is the first study to focus on sex differences in SSB consumption in intergenerational relationships, these findings still provide an interesting perspective for future research in other populations, including a larger sample across Chinese general population.
In our study, children's SSB intake would be affected by older siblings’ SSB consumption rather than that of younger brothers or sisters, which was consistent with a recent cross-sectional study in England [13]. O’Leary et al. [13] only found a correlation of intrahousehold SSB consumption between children of different ages, and because of the methodological limitations, the direction of causality is difficult to assess. The results of this study further determined the direction of the association. In the present study, the older children were already in adolescence (median age: 12 years), and younger children were still in prepubertal period (median age: 8 years). Adolescents have considerable autonomy and decision-making power regarding their dietary behavior [51]. Compared to their younger siblings, they prefer spending lots of time with their friends [52] and get pocket money [8] which may be used to purchase unhealthy food. For younger children, they tend to imitate older siblings to develop their dietary behavior [53]. In 2016, China officially ended the one-child policy, and in 2021, the government even encouraged reproductive-age women to have three births. More than 8 million second child were born in 2016, and 59.5% of newborns were second child in 2019 [54]. With the increasing number of multiple-child families in China, the influence of sibling’s effect cannot be ignored. For second child’s parents, who were likely raised in a single-child family and have little experience with siblings, and this makes education for multiple children has become a critical social issue requiring immediate attention. However, due to limitations imposed by the small sample size, our estimation results for sex differences in the relationships between siblings and children in SSB consumption were not reliably available (Table S5), still, our findings provided an interesting new direction for future research in dietary consumption.
Our study has several strengths, including its prospective nature to establish causal order, and the ability to adjust for a number of potential confounders both in children and in parents. A further advantage lies in the detailed exploration of SSB consumption in both fathers and mothers. Moreover, unlike other studies of children or adolescents, we noted sex differences in SSB intergenerational relationships, which may require more attention in the development of SSB reduction policies for children.
Nevertheless, some limitations should also be mentioned. First, though the amount of SSB intake in this study is consistent with that obtained in other studies of Chinese children and adults, the dietary assessment method of SSB has not been validated yet. And self-report of dietary data and the unavailability of energy intake data obtained through the food frequency questionnaire introduced the possibility of bias and underreporting. Second, as the CHNS has not regularly tested the consistency in the operation of investigators, there might be inadequacies with the quality of basic anthropometric measurements (height and weight). Third, though acceptance of initial invitation for study participants varied by area, we excluded participants who refused participation, which may have resulted in the selection of a more “health-conscious” study sample. Fourth, the sample size limited the extent of analysis which makes us unable to analyze the sex difference in siblings’ impact and in families with only one parent drinking SSB.
In conclusion, our study illustrated that parental SSB consumption and older siblings’ SSB intake, not younger siblings’ SSB intake, were prospectively associated with Chinese children’s SSB consumption. And in Chinese families, boys were more susceptible to their parents' SSB intake than girls, and fathers seemed to have more influence on children’s SSB consumption than mothers.
Data availability
The China Health and Nutrition Survey is an open-access resource, data are available at http://www.cpc.unc.edu/projects/china/data/datasets.
References
Guo H, Phung D, Chu C (2021) Sociodemographic, lifestyle, behavioral, and parental factors associated with sugar-sweetened beverage consumption in children in China. PLoS ONE 16(12):e0261199. https://doi.org/10.1371/journal.pone.0261199
Bleich SN, Vercammen KA (2018) The negative impact of sugar-sweetened beverages on children’s health: an update of the literature. BMC Obes 5:6. https://doi.org/10.1186/s40608-017-0178-9
Romanos-Nanclares A, Toledo E, Gardeazabal I, Jiménez-Moleón JJ, Martínez-González MA, Gea A (2019) Sugar-sweetened beverage consumption and incidence of breast cancer: the Seguimiento Universidad de Navarra (SUN) Project. Eur J Nutr 58(7):2875–2886. https://doi.org/10.1007/s00394-018-1839-2
Malik VS, Popkin BM, Bray GA, Després JP, Hu FB (2010) Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation 121(11):1356–1364. https://doi.org/10.1161/circulationaha.109.876185
Grimm GC, Harnack L, Story M (2004) Factors associated with soft drink consumption in school-aged children. J Am Diet Assoc 104(8):1244–1249. https://doi.org/10.1016/j.jada.2004.05.206
Greenberg RS, Ariza AJ, Binns HJ (2010) Activity and dietary habits of mothers and children: close ties. Clin Pediatr 49(11):1026–1032. https://doi.org/10.1177/0009922810375844
Bauer KW, Neumark-Sztainer D, Fulkerson JA, Hannan PJ, Story M (2011) Familial correlates of adolescent girls’ physical activity, television use, dietary intake, weight, and body composition. Int J Behav Nutr Phys Activ 8:25. https://doi.org/10.1186/1479-5868-8-25
van Ansem WJ, van Lenthe FJ, Schrijvers CT, Rodenburg G, van de Mheen D (2014) Socio-economic inequalities in children’s snack consumption and sugar-sweetened beverage consumption: the contribution of home environmental factors. Br J Nutr 112(3):467–476. https://doi.org/10.1017/s0007114514001007
Bogart LM, Elliott MN, Ober AJ, Klein DJ, Hawes-Dawson J, Cowgill BO, Uyeda K, Schuster MA (2017) Home sweet home: parent and home environmental factors in adolescent consumption of sugar-sweetened beverages. Acad Pediatr 17(5):529–536. https://doi.org/10.1016/j.acap.2017.01.015
Tasevska N, DeLia D, Lorts C, Yedidia M, Ohri-Vachaspati P (2017) Determinants of sugar-sweetened beverage consumption among low-income children: are there differences by race/ethnicity, age, and sex? J Acad Nutr Diet 117(12):1900–1920. https://doi.org/10.1016/j.jand.2017.03.013
Lundeen EA, Park S, Onufrak S, Cunningham S, Blanck HM (2018) Adolescent sugar-sweetened beverage intake is associated with parent intake, not knowledge of health risks. Am J Health Promot 32(8):1661–1670. https://doi.org/10.1177/0890117118763008
Imoisili OE, Park S, Lundeen EA, Yaroch AL, Blanck HM (2020) Daily adolescent sugar-sweetened beverage intake is associated with select adolescent, not parent, attitudes about limiting sugary drink and junk food intake. Am J Health Promot AJHP 34(1):76–82. https://doi.org/10.1177/0890117119868382
O’Leary C, Cummins S, Smith RD, Cornelsen L (2021) Like parent, like child: a cross-sectional study of intra-household consumption patterns of non-alcoholic beverages among British households with children. Public Health Nutr 25:1771–1779. https://doi.org/10.1017/s1368980021005061
Wong RSM, Yu EYT, Guo VY, Wan EY, Chin WY, Wong CKH, Fung CSC, Tung KTS, Wong WH, Ip P, Tiwari AFY, Lam CLK (2018) A prospective cohort study to investigate parental stress and child health in low-income Chinese families: protocol paper. BMJ Open 8(2):e018792. https://doi.org/10.1136/bmjopen-2017-018792
Inoura S, Shimane T, Kitagaki K, Wada K, Matsumoto T (2020) Parental drinking according to parental composition and adolescent binge drinking: findings from a nationwide high school survey in Japan. BMC Public Health 20(1):1878. https://doi.org/10.1186/s12889-020-09969-8
Huppertz C, Bartels M, Beijsterveldt CV, Boomsma DI, Hudziak JJ, Geus ED (2012) Effect of shared environmental factors on exercise behavior from age 7 to 12 years. Med Sci Sports Exerc 44(10):2025–2032
Riley MD, Hendrie GA, Baird DL (2019) Drink choice is important: beverages make a substantial contribution to energy, sugar, calcium and vitamin C intake among Australians. Nutrients 11(6):1389. https://doi.org/10.3390/nu11061389
Pinilla J, Lopez-Valcarcel BG, Urbanos-Garrido RM (2017) Estimating direct effects of parental occupation on Spaniards’ health by birth cohort. BMC Public Health 17(1):26. https://doi.org/10.1186/s12889-016-3997-6
Vanhelst J, Béghin L, Drumez E, Duhamel A, De Henauw S, Ruiz JR, Kafatos A, Manios Y, Widhalm K, Mauro B (2018) Adolescents’ diet quality in relation to their relatives’ and peers’ diet engagement and encouragement: the Healthy Lifestyle in Europe by Nutrition in Adolescence (HELENA) study. Public Health Nutr 21(17):3192–3201
Senguttuvan U, Whiteman SD, Jensen AC (2014) Family relationships and adolescents’ health attitudes and weight: the understudied role of sibling relationships. Fam Relat 63(3):384–396
Zhang B, Zhai F, Du S, Popkin BM (2014) The China health and nutrition survey, 1989–2011. Obes Rev 15:2–7
Description of CHNS design. http://www.cpc.unc.edu/projects/china.
China Health and Nutrition Survey. http://www.cpc.unc.edu/projects/china/data/datasets/longitudinal.
Cohen J (1992) A power primer. Psycholog Bull 112(1):155–159. https://doi.org/10.1037//0033-2909.112.1.155
Yuan YQ, Li F, Wu H, Wang YC, Chen JS, He GS, Li SG, Chen B (2018) Evaluation of the validity and reliability of the Chinese healthy eating index. Nutrients 10(2):114. https://doi.org/10.3390/nu10020114
Li Y, Wang DD, Ley SH, Vasanti M, Howard AG, He Y, Hu FB (2017) Time trends of dietary and lifestyle factors and their potential impact on diabetes burden in China. Diabetes Care 40(12):1685–1694. https://doi.org/10.2337/dc17-0571
Zhai F, Popkin BM, Ma L, Yu W, Guo X, Gao J, Ge K (1996) The evaluation of the 24-hour individual dietary recall method in China. J Hyg Res 25:51–56. https://doi.org/10.19813/j.cnki.weishengyanjiu.1996.s1.010 (in Chinese)
Bureau SS (2017) Sichuan Statistical Yearbook in 2017. Sichuan Statistical Bureau, Chengdu
Montagu M, Brožek JC (1960) A handbook of anthropometry
Min J, Xue H, Wang VHC, Li M, Wang Y (2017) Are single children more likely to be overweight or obese than those with siblings? The influence of China’s one-child policy on childhood obesity. Prevent Med 103:8–13. https://doi.org/10.1016/j.ypmed.2017.07.018
Li H, Ji C, Zong X, Zhang Y (2009) Growth curve of body mass index for children and adolescents aged 0–18 years in China. Chin J Pediatr 47(7):493–498
AbellanaSangra R, FarranCodina A (2015) The identification, impact and management of missing values and outlier data in nutritional epidemiology. Nutr Hospital 31(Suppl 3):189–195. https://doi.org/10.3305/nh.2015.31.sup3.8766
Pan XB, Wang HJ, Zhang B, Liu YL, Qi SF, Tian QB (2020) Plain water intake and association with the risk of overweight in the Chinese adult population: China Health and Nutrition Survey 2006–2011. J Epidemiol 30(3):128–135. https://doi.org/10.2188/jea.JE20180223
Willett WC, Howe GR, Kushi LH (1997) Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr 65(4 Suppl):1220S-1228S. https://doi.org/10.1093/ajcn/65.4.1220S (discussion 1229S-1231S)
Pearson N, Biddle SJ, Gorely T (2009) Family correlates of fruit and vegetable consumption in children and adolescents: a systematic review. Public Health Nutr 12(2):267–283. https://doi.org/10.1017/s1368980008002589
Wang Y, Beydoun MA, Li J, Liu Y, Moreno LA (2011) Do children and their parents eat a similar diet? Resemblance in child and parental dietary intake: systematic review and meta-analysis. J Epidemiol Commun Health 65(2):177–189. https://doi.org/10.1136/jech.2009.095901
Lai-Yeung TWL (2015) Hong Kong parents’ perceptions of the transference of food preparation skills. Int J Consum Stud 39(2):117–124. https://doi.org/10.1111/ijcs.12158
Mazarello Paes V, Hesketh K, O’Malley C, Moore H, Summerbell C, Griffin S, van Sluijs EM, Ong KK, Lakshman R (2015) Determinants of sugar-sweetened beverage consumption in young children: a systematic review. Obes Rev 16(11):903–913. https://doi.org/10.1111/obr.12310
Irwin BR, Speechley MR, Gilliland JA (2019) Assessing the relationship between water and nutrition knowledge and beverage consumption habits in children. Public Health Nutr 22(16):3035–3048. https://doi.org/10.1017/s1368980019000715
Blecher E, Liber AC, Drope JM, Nguyen B, Stoklosa M (2017) Global trends in the affordability of sugar-sweetened beverages, 1990–2016. Prevent Chronic Dis 14:E37. https://doi.org/10.5888/pcd14.160406
Li J, Feldman MW, Li S, Daily GC (2011) Rural household income and inequality under the Sloping Land Conversion Program in western China. Proc Nat Acad Sci USA 108(19):7721–7726. https://doi.org/10.1073/pnas.1101018108
Farmaki A, Christou P, Saveriades A, Spanou-Tripinioti E (2019) Perceptions of Pafos as European Capital of Culture: tourism stakeholder and resident perspectives. Int J Tour Res 21(2):234–244. https://doi.org/10.1002/jtr.2257
Kalavana TV, Maes S, De Gucht V (2010) Interpersonal and self-regulation determinants of healthy and unhealthy eating behavior in adolescents. J Health Psychol 15(1):44–52. https://doi.org/10.1177/1359105309345168
Ragelienė T, Grønhøj A (2020) The influence of peers’ and siblings’ on children’s and adolescents’ healthy eating behavior. A systematic literature review. Appetite 148:104592. https://doi.org/10.1016/j.appet.2020.104592
McCoy SS, Dimler LM, Samuels DV, Natsuaki MN (2019) Adolescent susceptibility to deviant peer pressure: does gender matter? Adolesc Res Rev 4:59–71. https://doi.org/10.1007/s40894-017-0071-2
Bašková M, Holubčíková J, Baška T (2017) Body-image dissatisfaction and weight-control behaviour in slovak adolescents. Central Eur J Public Health 25(3):216–221. https://doi.org/10.21101/cejph.a4724
Mäkinen M, Puukko-Viertomies LR, Lindberg N, Siimes MA, Aalberg V (2012) Body dissatisfaction and body mass in girls and boys transitioning from early to mid-adolescence: additional role of self-esteem and eating habits. BMC Psychiatry 12:35. https://doi.org/10.1186/1471-244x-12-35
Jago R, Wood L, Zahra J, Thompson JL, Sebire SJ (2015) Parental control, nurturance, self-efficacy, and screen viewing among 5- to 6-year-old children: a cross-sectional mediation analysis to inform potential behavior change strategies. Childhood Obes 11(2):139–147. https://doi.org/10.1089/chi.2014.0110
Bi X, Yang Y, Li H, Wang M, Zhang W, Deater-Deckard K (2018) Parenting styles and parent-adolescent relationships: the mediating roles of behavioral autonomy and parental authority. Front Psychol 9:2187. https://doi.org/10.3389/fpsyg.2018.02187
Yang MZ, Xue HM, Pan J, Libuda L, Muckelbauer R, Yang M, Quan L, Cheng G (2018) High protein intake along with paternal part-time employment is associated with higher body fat mass among girls from South China. Eur J Nutr 57(5):1845–1854. https://doi.org/10.1007/s00394-017-1468-1
Neufeld LM, Andrade EB, Ballonoff Suleiman A, Barker M, Beal T, Blum LS, Demmler KM, Dogra S, Hardy-Johnson P, Lahiri A, Larson N, Roberto CA, Rodríguez-Ramírez S, Sethi V, Shamah-Levy T, Strömmer S, Tumilowicz A, Weller S, Zou Z (2022) Food choice in transition: adolescent autonomy, agency, and the food environment. Lancet (London, England) 399(10320):185–197. https://doi.org/10.1016/s0140-6736(21)01687-1
Smit CR, de Leeuw RNH, Bevelander KE, Burk WJ, Buijzen M (2016) A social network-based intervention stimulating peer influence on children’s self-reported water consumption: a randomized control trial. Appetite 103:294–301. https://doi.org/10.1016/j.appet.2016.04.011
Golan M, Crow S (2004) Parents are key players in the prevention and treatment of weight-related problems. Nutr Rev 62(1):39–50. https://doi.org/10.1111/j.1753-4887.2004.tb00005.x
Y Z (2020) The growth rate of total population slowed down and the level of urbanization continued to increase. National Bureau of Statistics. http://www.stats.gov.cn/tjsj/sjjd/202001/t20200119_1723861.html.
Yearbook CS (2012) National Bureau of statistics of China. China Statistical Yearbook
Acknowledgements
This research uses data from China Health and Nutrition Survey (CHNS). The authors would like to thank all the participants in our study and the staff responsible for conducting the CHNS. And we are also grateful to the team at the National Institute for Nutrition and Health, Chinese Center for Disease Control and Prevention, the Carolina Population Center, University of North Carolina at Chapel Hill.
Funding
This study was supported by Study of Diet and Nutrition Assessment and Intervention Technology (No. 2020YFC2006300) from Active Health and Aging Technologic Solutions Major Project of National Key R&D Program.
Author information
Authors and Affiliations
Contributions
XTL conceived of and designed the study, conducted the statistical analysis, and drafted the manuscript; JYX, YJX and LZ reviewed and editing the data interpretation; LL contributed to the critical review of the manuscript; and GC designed the study, supervised the study process, and contributed to data interpretation and the critical review of the manuscript. All authors have seen and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
All participants provided their written informed consent. The China Health and Nutrition Survey (CHNS) study was conducted according to the Helsinki declaration and approved by the institutional review committees of the University of North Carolina at Chapel Hill and Chinese Center for Disease Control and Prevention.
Consent for publication
This manuscript is not being simultaneously submitted elsewhere and no portion of the data has been published elsewhere.
Conflict of interest
All authors declare that they have no conflict of interest.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, XT., Xiong, JY., Xu, YJ. et al. Prospective association of family members’ sugar-sweetened beverages intake with children’s sugar-sweetened beverages consumption in China. Eur J Nutr 62, 175–184 (2023). https://doi.org/10.1007/s00394-022-02971-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-022-02971-3