
Abstract
Purposes
Bowel resection in patients with Crohn’s disease (CD) has a high reported rate of postoperative complications and surgical recurrence. A macroscopically normal resection margin is recommended in CD surgery as wider margins do not translate in reduced recurrence rates. The aim of this study was to evaluate the association between resection margin status and anastomotic complications following ileocaecal resection for primary CD.
Methods
All patients treated with ileocaecal resection for primary CD from 2010 to 2018 were included in this retrospective observational study. Emergency operations and recurrent CD were excluded. Patients in whom an anastomosis was not fashioned at the time of the surgery were also excluded. Histopathology data collected included macroscopic description, presence of macroscopic and microscopic involvement of the proximal and distal resection margins. The primary outcome was the rate of positive resection margin in patients who developed anastomotic complications (anastomotic leaks and intra-abdominal collections), and the secondary outcomes were overall complications rate, length of hospital stay, reoperations and rehospitalisation within 30 days.
Results
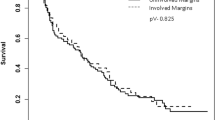
A total of 104 patients were included. The proximal resection margin was microscopically involved in 19 patients (18.2%). Ten patients (9.6%) developed intra-abdominal anastomotic related complications, with 5 patients out of 10 (50%) in the group of postoperative anastomotic complications having a positive microscopic proximal margin at histology, compared to 14 patients (14.9%) in the group that did not develop anastomotic complications (p < 0.0001).
Conclusions
Microscopic involvement of the proximal resection margin is more frequent in patients who develop postoperative anastomotic complications following elective ileocaecal resection for primary CD.
Similar content being viewed by others


References
Shaffer VO, Wexner SD (2013) Surgical management of Crohn's disease. Langenbeck's Arch Surg 398:13–27
Dasari BV, McKay D, Gardiner K (2011) Laparoscopic versus open surgery for small bowel Crohn's disease. Cochrane Database Syst Rev 19:CD006956
Fumery M, Seksik P, Chirica M et al (2015) Postoperative complications after Ileo-Caecal resection for Crohn's disease: a prospective multicentre study gastroenterology. 148(4) Suppl 1:S132–S133
Alves A, Panis Y, Bouhnik Y, Pocard M, Vicaut E, Valleur P (2007) Risk factors for intra-abdominal septic complications after a first ileocecal resection for Crohn’s disease: a multivariate analysis in 161 consecutive patients. Dis Colon Rectum 50:331–336
Lau C, Dubinsky M, Melmed G et al (2013) Higher preoperative serum biologic levels are associated with postoperative complications in Crohn's disease patients. Gastroenterology 144(5 Suppl 1):S190–S190
Yamamoto T, Allan RN, Keighley MR (2000) Risk factors for intra abdominal sepsis after surgery in Crohn’s disease. Dis Colon Rectum 43:1141–1145
Yamamoto T, Keighley MR (1999) The association of cigarette smoking with a high risk of recurrence after ileocolonic resection for ileocecal Crohn's disease. Surg Today 29(6):579–580
Gordon PH, Nivatvongs S (2007) New York, NY: Informa healthcare. Crohn's Dis 820–907
Olaison G, Smedh K, Sjodahl R (1992) Natural course of Crohn's disease after ileocolic resection: endoscopically visualised ileal ulcers preceding symptoms. Gut 33(3):331–335
He X, Chen Z, Huang J, Lian L, Rouniyar S, Wu X, Lan P (2014) Stapled side-to-side anastomosis might be better than handsewn end-to-end anastomosis in ileocolic resection for Crohn’s disease: a meta-analysis. Dig Dis Sci 59(7):1544–1551
Fazio VW, Marchetti F, Church M et al (1996) Effect of resection margins on the recurrence of Crohn's disease in the small bowel. A randomized controlled trial. Ann Surg 224(4):563–573
Buisson A, Chevaux JB, Allen PB, Bommelaer G, Peyrin-Biroulet L (2012) Review article: the natural history of postoperative Crohn's disease recurrence. Aliment Pharmacol Ther 35(6):625–633
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP (2008) STROBE initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 61(4):344–349
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Uchino M, Ikeuchi H, Bando T, Matsuoka H, Takahashi Y, Takesue Y, Matsumoto T, Tomita N (2012) Risk factors for short bowel syndrome in patients with Crohn's disease. Surg Today 42(5):447–452
Nightingale JM, Lennard-Jones JE (1995) Adult patients with a short bowel due to Crohn's disease often start with a short normal bowel. Eur J Gastroenterol Hepatol 7(10):989–991
Pariente B, Mary JY, Danese S, Chowers Y, de Cruz P, D’Haens G, Loftus EV Jr, Louis E, Panés J, Schölmerich J, Schreiber S, Vecchi M, Branche J, Bruining D, Fiorino G, Herzog M, Kamm MA, Klein A, Lewin M, Meunier P, Ordas I, Strauch U, Tontini GE, Zagdanski AM, Bonifacio C, Rimola J, Nachury M, Leroy C, Sandborn W, Colombel JF, Cosnes J (2015) Development of the Lémann index to assess digestive tract damage in patients with Crohn's disease. Gastroenterology 148:52–63
Morar PS, Hollingshead J, Bemelman W, Sevdalis N, Pinkney T, Wilson G, Dunlop M, Davies RJ, Guy R, Fearnhead N, Brown S, Warusavitarne J, Edwards C, Faiz O (2017) Establishing key performance indicators [KPIs] and their importance for the surgical Management of Inflammatory Bowel Disease-Results from a pan-European, Delphi consensus study. J Crohns Colitis 11(11):1362–1368
Setoodeh S, Liu L, Boukhar SA, Singal AG, Westerhoff M, Waljee AK, Ahmed T, Gopal P (2019) The clinical significance of Crohn disease activity at resection margins. Arch Pathol Lab Med 143(4):505–509
Karesen R, Serch-Hanssen A, Thoresen BO, Hertzberg J (1981) Crohn’s disease: long-term results of surgical treatment. Scand J Gastroenterol 16(1):57–64
Heimann TM, Greenstein AJ, Lewis B, Kaufman D, Heimann DM, Aufses AH Jr (1993) Prediction of early symptomatic recurrence after intestinal resection in Crohn’s disease. Ann Surg 218(3):294–298 discussion 298–299
Adloff M, Arnaud JP, Ollier JC (1987) Does the histologic appearance at the margin of resection affect the postoperative recurrence rate in Crohn’s disease? Am Surg 53(10):543–546
Kotanagi H, Kramer K, Fazio VW, Petras RE (1991) Do microscopic abnormalities at resection margins correlate with increased anastomotic recurrence in Crohn’s disease?: retrospective analysis of 100 cases. Dis Colon Rectum 34(10):909–916
Bemelman WA, Warusavitarne J, Sampietro GM et al (2018) ECCO-ESCP consensus on surgery for Crohn’s disease. J Crohn's Colitis 12(1):1–16
Ryan JM, Rogers AC, O'Toole A, Burke JP (2019) Meta-analysis of histological margin positivity in the prediction of recurrence after Crohn's resection. Dis Colon Rectum 62(7):882–892
Coffey JC, Kiernan MG, Sahebally SM et al (2018) Inclusion of the mesentery in ileocolic resection for Crohn’s disease is associated with reduced surgical recurrence. J Crohns Colitis 12(10):1139–1150
Buskens CJ, de Groof EJ, Bemelman WA, Wildenberg ME (2017) The role of the mesentery in Crohn's disease. Lancet Gastroenterol Hepatol 2(4):245–246
IBD Standards Group (2013) Standards for the healthcare of people who have inflammatory bowel disease [IBD]. 2013 update. Oyster Healthcare Communications, St Albans
NICE Quality Standard [QS81]—Inflammatory Bowel Disease. http://www.nice.org.uk/guidance/qs81/chapter/quality-statement-2-multidisciplinary-team-support. Accessed 10 Jan 2019
Calvet X, Panes J, Alfaro N et al (2014) Delphi consensus statement: quality indicators for inflammatory bowel disease comprehensive care units. J Crohns Colitis 8:240–251
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study is conducted in accordance with the principles of the Declaration of Helsinki and ‘good clinical practice’ guidelines. Informed consent has been obtained from the patients.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Garofalo, E., Lucarini, A., Flashman, K.G. et al. A positive proximal resection margin is associated with anastomotic complications following primary ileocaecal resection for Crohn’s disease. Int J Colorectal Dis 34, 1585–1590 (2019). https://doi.org/10.1007/s00384-019-03358-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-019-03358-3