
Abstract
The aim of the study was to investigate the effects of hypovitaminosis D on pain, quality of life (QoL) and nerve conduction studies (NCSs) in patients with chronic widespread pain (CWP). We randomly selected 83 female patients with CWP according to their vitamin D levels in this cross-sectional study. Patients were divided into two groups as sufficient vitamin D level (above 20 ng/ml) and deficient vitamin D level (below 20 ng/ml, hypovitaminosis D). Various pain scales and Nottingham Health Profile (NHP) were used. NCSs were also done. In patients with hypovitaminosis D, there were significantly higher pain scores for all scales (p value range 0.002–0.027). The subscale and total NHP scores were significantly higher in hypovitaminosis D group (p = 0.048–0.001) except social isolation subscale (p = 0.553). Vitamin D levels were in negative correlation with right and left median and/or ulnar motor nerve amplitudes, left tibial motor amplitude. This study confirm that hypovitaminosis D is related with higher pain intensity and lower QoL scores in patients with CWP when compared with control group. Additionally, we identified for the first time that there were negative correlations between vitamin D levels and some findings of NCSs.
Similar content being viewed by others

Introduction
Vitamin D is produced in the skin by converting 7-dehydrocholesterol to pre-vitamin D3 under the influence of ultraviolet-B radiation. It is a secosteroid type hormone and isomerized to vitamin D by a thermal energy [1]. It becomes biologically active with further sunlight exposure [1]. Hypovitaminosis D is a worldwide pandemic, and the principal reason is inadequate synthesis (i.e., indoor workplace, wearing whole body covering clothes, geographical disadvantages) [2]. Recent studies indicate that hypovitaminosis D may be related with many cancer types, chronic pain, autoimmune diseases, hypertension, growth and development delay in children [3, 4].
Musculoskeletal complaints in various forms (regional pain, limb pain, joint pain, chronic widespread pain) are one of the major reasons for outpatient consultations [5]. Vitamin D is effective in musculoskeletal system health with vitamin D receptor and calcium-phosphorus metabolism [6]. Relationship between hypovitaminosis D and muscle weakness has also been shown. Besides, proximal muscle weakness is related with increased imbalance and resulted with falls [7]. Vitamin D deficiency is also associated with bone mineralization defects in which, isolated or generalized musculoskeletal pain complaints may be seen especially due to osteomalacia [3]. Those patients can be misdiagnosed in clinical settings as fibromyalgia syndrome, osteoarthritis, inflammatory arthritis or chronic fatigue syndrome [3, 8]. Hypovitaminosis D may also be resulted in hyperinnervation and hypersensitivity in nerve fibers which are carrying pain sensation and cause increased pain perception in already existing pathology [9]. Vitamin D is essential in brain homeostasis because it is a neuroactive compound (neurosteroid) [10]. It has action on nerve growth factors and has neuroprotective effects [10].
Pain is defined as by International Association for the Study of Pain as “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” [11]. Pain which persists more than 3 months is defined as chronic pain and it is more common among women and can be seen in one in every five people [12]. Relationship with hypovitaminosis D and various pain types including chronic widespread pain have also been implicated [13–16]. Silva et al. [17] also reveal that subjects with hypovitaminosis D was reported more frequent and severe back pain when compared with control group. In a recent small trial, the ameliorative effect of vitamin D supplementation on diffuse musculoskeletal pain and quality of life was evident [18] and those results were consistent with the previous studies [19].
The aim of the study was to demonstrate the effects of vitamin D deficiency on pain characteristics, quality of life and nerve conduction studies (NCSs) in patients with chronic widespread pain.
Materials and method
Patients
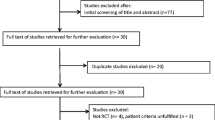
Two hundred and sixteen patients with pain complaint were admitted to Physical Medicine and Rehabilitation outpatient clinics during September 2013 and February 2014. They were diagnosed with chronic widespread pain and the ones who had comorbid conditions that could effect the motor and sensory NCSs (i.e., diabetes, thyroid problems, and taking cancer-related treatment) were not included in the study. At the same time, medical history and physical examination were performed. The patients with entrapment neuropathy (i.e., Carpal tunnel syndrome, ulnar entrapment, tarsal tunnel syndrome) history were also not included in the study. Remaining 83 female patients who were convenient and accepted to participate in this study were included consecutively. Additionally, they were divided into age-matched 2 subgroups according to their Vitamin D levels.
Serum vitamin D level measurements and other biochemical parameters
Serum 25-hydroxyvitamin D levels were determined by chemiluminescence using Nichols Advantage competitive binding assay (San Juan Capistrano, California, USA) [20]. According to general agreement, 25-hydroxyvitamin D concentration 50 nmol/L, or 20 ng/mL, is an indication of vitamin D deficiency, a 25-hydroxyvitamin D concentration of 51–74 nmol/L, or 21–29 ng/mL, is considered to indicate insufficiency; concentrations 30 ng/mL are considered to be sufficiency [21]. A 25-hydroxyvitamin D level below 20 ng/mL was considered to indicate vitamin D deficiency in our study. Above this limit was accepted as non-deficiency state. Serum calcium, ionized calcium, phosphorus, alkaline phosphatase and parathyroid hormone levels were also evaluated.
Pain assessment
Visual Analog Scale (VAS), Verbal Rating Scale (VRS), Numeric Rating Scale (NRS) and Face Pain Scale (FPS) were used to assess pain. The VAS is presented as a 10-cm horizontal and vertical line. It goes from “no pain” to “worst imaginable pain” between two ends of the line [22]. VRS is another tool to evaluate pain intensity [23]. VRS consists of mostly five or six adjectives that describe different levels of pain degree. The commonly used words for gradual intensities are as follows: no pain, mild pain, moderate pain, severe or intense pain, AND pain as bad as it could be. The patient is asked to select the best one that describes his or her pain intensity in a questionnaire. NRS is a 11-point scale which is between no pain and worst pain. The NRS is asked both graphically and verbally [24]. FPS includes 6 faces in horizontal line is scored from 0 to 10, that ranged from smiling face to the crying face according to pain intensity [25].
Quality of life
The Nottingham Health Profile (NHP) is widely used as a generic quality of life questionnaire which is relatively quick and easy to complete. The NHP has been used in patients with osteoarthritis, and various chronic pain complaints [26–28] and determined appropriate for our patients. The validity and reliability for Turkish population were made by Kucukdeveci et al. [29]. It measures the health-related QoL in patients and focuses on self-perceived physical, emotional and social health status [30]. The NHP is suitable for epidemiological studies of health and disease [31] and it has two parts. In the first part, perceived functional status measured by requiring a “yes” or “no” answer to 38 questions. It has 6 dimensions: energy (3 items), pain (8 items), emotional reaction (9 items), sleeping (5 items) social isolation (5 items), and physical mobility (8 items). Each dimension has a score in the range between 0 and 100 where zero indicates good health and 100 indicates poor health and each statement is scored using weighted values. The second part of the questionnaire could also be used separately, and it is about the effects of patient’s functional health status on 7 areas of daily life [30] which was not used in the current study. The NHP and questionnaire form and pain scales were administrated face to face by interviewers.
Nerve conduction studies
Electroneurography was applied in order to see the effect of hypovitaminosis D on motor and sensory NCSs. Median and ulnar motor and sensory nerves from upper extremities and peroneal, tibial and sural nerves from lower extremities were evaluated bilaterally. NCSs were performed with Medtronic–Keypoint (Denmark, 2007) device by the physiatrist. All studies were done under normal conditions (i.e., standard room temperature was around 25 °C, and limb temperature was around 32 °C).
Motor NCSs
Median and ulnar motor nerve distal latencies, median and ulnar motor nerve conduction velocity, compound muscle action potential (CMAP) amplitudes at the wrist and elbow were measured. Median motor NCSs were recorded with surface electrodes from abductor pollicis brevis muscle and ulnar motor NCSs were also recorded with cup electrodes from abductor digiti minimi. The stimulation points were proximal to the carpal tunnel for median nerve and Guyon canal for ulnar nerve with standard distance of 8 cm. Tibial motor NCSs were recorded with surface electrodes from abductor hallucis longus muscle and stimulation points were ankle and knee. Peroneal motor NCSs were also recorded with surface electrodes from extansor pollicis brevis muscle and stimulation points were ankle and below knee (fibular head) and above knee (poplitea).
Sensory NCSs
Median sensory NCSs were recorded with cup electrodes from 3rd digit antidromically with standard distance of 14 cm. Ulnar sensory NCSs were recorded from 5th digit with standard distance of 12 cm. Sural NCSs were recorded from external malleolus and stimulation was given 14 cm at midcalf point. For all sensory NCSs, distal latency, sensory nerve action potential amplitude and sensory nerve conduction velocity were evaluated. The latencies were marked at the onset of first negative peak, and the amplitudes were determined from peak to peak [32].
Ethics
The procedures followed were in accordance with the ethical standards of the Helsinki Declaration of 1975, as revised in 1983. This study was approved by Marmara University School of Medicine Local Ethics Committee and informed consent was obtained from subjects.
Statistical analysis
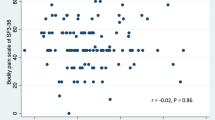
All analyses were performed using Statistical Package for the Social Science Program for Windows version 20.0. The main characteristics of patients were evaluated with descriptive and analytical statistics. Comparison of the mean values was performed with independent samples t tests, and categorical values were analyzed with Chi-square tests. p values lower than 0.05 was accepted as statistically significant. Data were expressed as mean ± standard deviation (mean ± SD) or median with minimum–maximum values. Normal distribution of continuous variables was tested with Kolmogorov–Smirnov test. Pearson’s correlations were used to determine if two variables are linearly related to each other.
Results
In this study, we recruited age and body mass index adjusted 83 female patients with musculoskeletal pain complaints. They were referred from physical medicine and rehabilitation outpatient clinic to biochemistry laboratory. According to vitamin D level, the patients were divided into two groups as vitamin D “deficient” and “non-deficient”. The demographic data was shown in Table 1.
When vitamin D groups compared, there was no difference in serum Ca, iCa, P, ALP levels; however, PTH levels were higher in hypovitaminosis D group when compared with control. There was also a negative correlation between PTH and vitamin D levels (p = 0.028, r = −0.308*). However, there was no relation between serum Ca, iCa, P, ALP and vitamin D levels.
Pain
The pain characteristics of the patients were summarized in Table 2. Patients with lower vitamin D level reported higher pain scores for all scales (NPS, FPS, VAS-horizontal, VAS-vertical) (p = 0.002–0.027) (statistical power: 91.4). There was no difference between horizontal and vertical VAS scores.
The frequency of pain was 53.9 % continuous, 14.5 % more than 2 times per day, 11.2 % 1–2 times per day and 13.2 % more than 2 times per week. Acute onset pain was seen in 58.4 %, pain increased with movement was 32.5 %, gradually increased pain was 9.1 %. The pain intensity was intractable in 6.3 %, very severe in 21.3 %, severe in 20 %, moderate in 50 %, and mild in 2.5 % of the patients.
Quality of life
Nottingham Health Profile score was used to assess quality of life in patients. The total and subscale comparison of the scores according to vitamin D levels were given in Table 3 (statistical power: 95.2). The subscale and total NHP scores were significantly higher in patients with lower vitamin D level (p = 0.05–0.001) except social isolation subscale (p = 0.553).
Nerve conduction studies
In the motor NCSs, there were increases in bilateral median and ulnar motor nerve amplitudes and left tibial motor nerve amplitudes in hypovitaminosis D group, and delay in bilateral ulnar motor and left tibial motor nerve latencies. Also there were decreases in left ulnar and right peroneal motor nerve conduction velocities (Table 4) (statistical power: 86.2). In the sensory NCSs, there was no difference among vitamin D groups.
There were 22 patients with carpal tunnel syndrome, 2 patients with ulnar nerve entrapment and 1 polyneuropathy according to electroneuromyography (ENMG) studies. There was no statistical significance between two groups according to nerve involvements (Table 5).
Discussion
Vitamin D deficiency is a pandemic and has many negative health-related consequences [3]. The desired serum levels are above 30 ng/ml [3]. Inadequate sun exposure is the main reason of hypovitaminosis D. Chronic widespread pain is one of the most difficult symptom to manage in clinical settings. There are several studies which indicate relationship between hypovitaminosis D and increased pain symptoms [4, 13–16]. In this study, both control and hypovitaminosis D group had chronic widespread pain. However, significant higher pain scores in various scales of hypovitaminosis D group than control group were obtained. This may indicate bone mineralization defect due to inadequate calcium phosphate levels caused by hypovitaminosis D. One of the probable mechanism is expanding collagen matrix of the bone causes outward pressure under periostal covering [15]. This increase in pressure may cause pain sensation in that area which is richly innervated by sensory nerve fibers [15].
Quality of life assessments are becoming very important in the evaluation of the effects of medical interventions [33]. The total and subscale NHP scores were negatively effected in hypovitaminosis D group when compared with control group except in social isolation subscale. This can be related with pain intensity. Wichert et al. [14] indicated that serum vitamin D concentrations below 20 ng/ml were associated with poorer physical performance and a greater decline in physical performance in both gender. The uneffected participation to social life may indicate that the patients can find a way to manage the unwanted effects of pain. Besides, sleep disturbances were also implicated in hypovitaminosis D [34]. Le Goaziou et al. [18] revealed that vitamin D replacement has positive impact on quality of life and pain complaints of patients with low vitamin D levels. On the contrary, there are also some quite few studies which are unable to show the link between hypovitaminosis D and lower quality of life with different types of questionnaires [35].
In this study, effect of hypovitaminosis D in patients with chronic widespread pain to the NCSs and relation with peripheral neuropathy were evaluated first time. In the NCSs, there were increases in motor nerve amplitudes of median, ulnar and tibial nerves in hypovitaminosis D group and delay in ulnar and tibial nerve latency and decrease in ulnar and peroneal motor nerve conduction velocities. The most important findings of this study were motor nerve involvement without any effect on sensory nerves and significant ulnar motor nerve involvement in every segments (wrist, below and above elbow). Additionally, there were median, tibial and peroneal motor nerve involvements.
Although some studies reveal relationship between hypovitaminosis D and diabetic polyneuropathy [36, 37], it is not relevant in normal populations. Diabetic patients were excluded from the present study, and there was no relation between peripheral neuropathy and hypovitaminosis D. Controversially, there were increased motor nerve amplitudes in hypovitaminosis D group.
Vitamin D is a neuroactive steroid and induces nerve growth factor. Thus, low levels of vitamin D can be related with neuritis and decrease in pain perception threshold. This can explain the obtained high scores in hypovitaminosis D group. Chabas et al. [38] examined the effect of vitamin D2 treatment on axon regeneration after peripheral (peroneal) nerve injury in rats. They suggest that the treatments enhanced the formation of new axons, besides increased axon diameter and improved sensory responses to metabolic stimulation Cekic et al. [39].
The clinical interpretation and underlying mechanism of some of the increased CMAP amplitudes in hypovitaminosis D group can not be explained with our current knowledge. In the study done by Akyuz et al. (1989, unpublished data), efficacy of pain on both central and peripheral nervous system had been assessed with ENMG and somatosensory evoked potentials (SEPs). In that study, 43 patients with unilateral undiagnosed upper extremity pain were evaluated with ENMG and SEPs. Three patients were diagnosed with carpal tunnel syndrome, besides cortical response obtained from the region with pain (Cc-FZ recording) had higher amplitude than normal values. Although it was not clarified, with increasing amplitude, the presentation area of pain was also thought to be amplified in the brain. Akyuz et al. [40] also found in their following studies that stimulating large diameter fibers with transcutaneous electrical nerve stimulation parameters for inhibition of pain caused decreased amplitude in cortical response which depends on Melzack and Wall’s gate control theory [41]. According to their theory, small diameter fibers carrying pain can be blocked at the spinal cord level if the large diameter fibers are stimulated enough. In the point of perception and presentation of pain, there are several studies about recorded evoked potentials following painful stimuli which are given by laser [42–44].
In the present study, it has been thought that there can be modification in pain perception of peripheral nerves and much more fibers can be fired easily in the presence of hypovitaminosis D. However, it can not be explained with the current knowledge that why only motor nerves involved. There are also some questions emerged for patients with pain. “Is there any reorganization in peripheral nervous system for pain presentation?”, “Does this increase in amplitudes of motor nerves show active role of vitamin D in pain conduction?”.
This study is the pioneer study which investigated the relationship between vitamin D level and NCSs and revealed this phenomenon. However, in order to obtain more precise results larger group studies are needed in which both men and women included. It can not be clarified with the current knowledge that how long have been the patients suffering from hypovitaminosis D. This is one of the main limitations of this study. Right interpretation of the electrophysiological findings with further studies, before and after vitamin D replacement may help to understand and interpret the findings of NCSs.
References
Holick M (2004) Vitamin D: importance in the prevention of cancers, type 1 diabetes, heart disease and osteoporosis. Am J Clin Nutr 79:362–371
Nair R, Maseeh A (2012) Vitamin D: the “sunshine” vitamin. J Pharmacol Pharmacother 3(2):118–126. doi:10.4103/0976-500X.95506
Holick M (2008) Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr 87(Suppl):1080S–1086S
Plotnikoff GA, Quigley JM (2003) Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin Proc 78(12):1463–1470
Main CJ, Williams AC (2002) ABC of psychological medicine: musculoskeletal pain. BMJ 325:534–537
Hamilton B (2010) Vitamin D and human skeletal muscle. Scand J Med Sci Sports 20:182–190. doi:10.1111/j.1600-0838.2009.01016.x
Broe KE, Chen TC, Weinberg J, Bischoff-Ferrari HA, Holick MF, Kiel DP (2007) A higher dose of vitamin d reduces the risk of falls in nursing home residents: a randomized, multiple-dose study. J Am Geriatr Soc 55(2):234–239
Sezer N, Tomruk-Sutbeyaz S, Kibar S et al (2009) Evaluation of quality of life and its determinants in postmenopausal and senile osteoporotic women. J PMR Sci 12:19–25
Tague SE, Clarke GL, Winter MK, McCarson KE, Wright DE, Smith PG (2011) Vitamin D deficiency promotes skeletal muscle hypersensitivity and sensory hyperinnervation. J Neurosci 31(39):13728–13738. doi:10.1523/JNEUROSCI.3637-11.2011
Kiraly SJ, Kiraly MA, Hawe RD, Makhani N (2006) Vitamin D as a neuroactive substance: review. ScientificWorldJournal 6:125–139
International Association for the Study of Pain (IASP) (1994) Task force on taxonomy part III. Pain terms. A current list with definitions and notes on usage. In: Merskey H, Bogduk N (eds) Classification of chronic pain, 2nd edn. IASP Press, Seattle, WA, pp. 209–214. [Available at http://www.iasp-pain.org. Accessed March 30, 2014]
Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D (2006) Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain 10:287–333
Lotfi A, Abdel-Nasser AM, Hamdy A, Omran AA, El-Rehany MA (2007) Hypovitaminosis D in female patients with chronic low back pain. Clin Rheumatol 26(11):1895–1901
Wicherts IS, van Schoor NM, Boeke AJ, Visser M, Deeg DJ, Smit J, Knol DL, Lips P (2007) Vitamin D status predicts physical performance and its decline in older persons. J Clin Endocrinol Metab 92(6):2058–2065
Mascarenhas C, Mobarhan S (2004) Hypovitaminosis D-induced pain. Nutr Rev 62:354–359
Gloth FM, Lindsay JM, Zelesnick LB, Greenough WB (1991) Can vitamin D deficiency produce an unusual pain syndrome. Arch Intern Med 151:1662–1664
E Silva AV, Lacativa PG, Russo LA, de Gregório LH, Pinheiro RA, Marinheiro LP (2013) Association of back pain with hypovitaminosis d in postmenopausal women with low bone mass. BMC Musculoskelet Disord 14(1):184. doi:10.1186/1471-2474-14-184
Le Goaziou MF, Kellou N, Flori M, Perdrix C, Dupraz C, Bodier E, Souweine G (2014) Vitamin D supplementation for diffuse musculoskeletal pain: results of a before-and-after study. Eur J Gen Pract 20(1):3–9
Heath KM, Elovic EP (2006) Vitamin D deficiency: implications in the rehabilitation setting. Am J Phys Med Rehabil 85(11):916–923
Ozkan B, Hatun S, Bereket A (2012) Vitamin D intoxication. Turk J Pediatr 54(2):93–98
Holick MF (2007) Vitamin D deficiency. N Engl J Med 357:266–281
Hawker GA, Mian S, Kendzerska T, French M (2011) Measures of adult pain: visual analog scale for pain (VAS pain), numeric rating scale for pain (NRS pain), McGill pain questionnaire (MPQ), short-form McGill pain questionnaire (SF-MPQ), chronic pain grade scale (CPGS), short form-36 bodily pain scale (SF-36 BPS), and measure of intermittent and constant osteoarthritis pain (ICOAP). Arthritis Care Res (Hoboken) 63(Suppl 11):S240–S252. doi:10.1002/acr.20543
Mannion AF, Balagué F, Pellisé F, Cedraschi C (2007) Pain measurement in patients with low back pain. Nat Clin Pract Rheumatol 3(11):610–618
Williamson A, Hoggart B (2005) Pain: a review of three commonly used pain rating scales. J Clin Nurs 14(7):798–804
Wong DL, Baker CM (1988) Pain in children: comparison of assessment scales. Pediatr Nurs 14(1):9–17
Yildiz N, Topuz O, Gungen GO, Deniz S, Alkan H, Ardic F (2010) Health-related quality of life (Nottingham Health Profile) in knee osteoarthritis: correlation with clinical variables and self-reported disability. Rheumatol Int 30(12):1595–1600. doi:10.1007/s00296-009-1195-x
Ordu Gokkaya NK, Gokce-Kutsal Y, Borman P, Ceceli E, Dogan A, Eyigor S, Karapolat H (2012) Geriatric rehabilitation research group of Turkish society of physical medicine and rehabilitation. Pain and quality of life (QoL) in elderly: the Turkish experience. Arch Gerontol Geriatr 55(2):357–362
Atalay NS, Sahin F, Atalay A, Akkaya N (2013) Comparison of efficacy of neural therapy and physical therapy in chronic low back pain. Afr J Tradit Complement Altern Med 10(3):431–435
Küçükdeveci AA, McKenna SP, Kutlay S, Gürsel Y, Whalley D, Arasıl T (2000) The development and psychometric assessment of the Turkish version of the Nottingham Health Profile. Int J Rehabil Res 23:31–38
European Group for Quality of Life Assessment and Health Measurement (1993) European guide to the Nottingham health profile. Brookwood Medical Publications, Brookwood (UK)
Hunt SM, McEwan T (1980) The development of a subjective health indicator. Social Health Illn 2:231–246
Yagci I, Gunduz OH, Sancak S, Agirman M, Mesci E, Akyuz G (2010) Comparative electrophysiological techniques in the diagnosis of carpal tunnel syndrome in patients with diabetic polyneuropathy. Diabetes Res Clin Pract 88(2):157–163. doi:10.1016/j.diabres.2010.02.011
Unalan D, Soyuer F, Ozturk A (2009) Should the Nottingham Health Profile or the Short Form-36 be given preference in stroke? Neurosciences 14(1):45–52
McCarty DE, Chesson AL Jr, Jain SK, Marino AA (2013) The link between vitamin D metabolism and sleep medicine. Sleep Med Rev. doi:10.1016/j.smrv.2013.07.001
Civelek GM, Pekyavas NO, Cetin N, Cosar SN, Karatas M (2014) Association of vitamin D deficiency with muscle strength and quality of life in postmenopausal women. Climacteric 17(4):472–477. doi:10.3109/13697137.2014.898265
Bell DS (2012) Reversal of the symptoms of diabetic neuropathy through correction of vitamin D deficiency in a type 1 diabetic patient. Case Rep Endocrinol. doi:10.1155/2012/165056
Shehab D, Al-Jarallah K, Mojiminiyi OA, Al Mohamedy H, Abdella NA (2012) Does vitamin D deficiency play a role in peripheral neuropathy in type 2 diabetes? Diabet Med 29(1):43–49. doi:10.1111/j.1464-5491.2011.03510.x
Chabas JF, Alluin O, Rao G, Garcia S, Lavaut MN, Risso JJ, Legre R, Magalon G, Khrestchatisky M, Marqueste T, Decherchi P, Feron F (2008) Vitamin D2 potentiates axon regeneration. J Neurotrauma 25:1247–1256. doi:10.1089/neu.2008.0593
Cekic M, Sayeed I, Stein DG (2009) Combination treatment with progesterone and vitamin D hormone may be more effective than monotherapy for nervous system injury and disease. Front Neuroendocrinol 30(2):158–172. doi:10.1016/j.yfrne.2009.04.002
Akyüz G, Güven Z, Ozaras N, Kayhan O (1995) The effect of conventional transcutaneous electrical nerve stimulation on somatosensory evoked potentials. Electromyogr Clin Neurophysiol 35(6):371–376
Melzack R, Wall PD (1965) Pain mechanisms: a new theory. Science 150(3699):971–979
Garcia-Larrea L (2012) Objective pain diagnostics: clinical neurophysiology. Neurophysiol Clin 42(4):187–197. doi:10.1016/j.neucli.2012.03.001
Pazzaglia C, Valeriani M (2009) Brain-evoked potentials as a tool for diagnosing neuropathic pain. Expert Rev Neurother 9(5):759–771. doi:10.1586/ern.09.16
Conflict of interest
We certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kuru, P., Akyuz, G., Yagci, I. et al. Hypovitaminosis D in widespread pain: its effect on pain perception, quality of life and nerve conduction studies. Rheumatol Int 35, 315–322 (2015). https://doi.org/10.1007/s00296-014-3099-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-014-3099-7