
Abstract
Purpose
Infective endocarditis (IE) is widely underdiagnosed or diagnosed after a major delay. The diagnosis is currently based on the modified DUKE criteria, where the only validated imaging technique is echocardiography, and remains challenging especially in patients with an implantable cardiac device. The aim of this study was to assess the incremental diagnostic role of 18F-FDG PET/CT in patients with an implanted cardiac device and suspected IE.
Methods
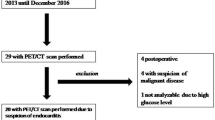
We prospectively analysed 27 consecutive patients with an implantable device evaluated for suspected device-related IE between January 2011 and June 2013. The diagnostic probability of IE was defined at presentation according to the modified DUKE criteria. PET/CT was performed as soon as possible following the clinical suspicion of IE. Patients then underwent medical or surgical treatment based on the overall clinical evaluation. During follow-up, we considered: lead cultures in patients who underwent extraction, direct inspection and lead cultures in those who underwent surgery, and a clinical/instrumental reevaluation after at least 6 months in patients who received antimicrobial treatment or had an alternative diagnosis and were not treated for IE. After the follow-up period, the diagnosis was systematically reviewed by the multidisciplinary team using the modified DUKE criteria and considering the new findings.
Results
Among the ten patients with a positive PET/CT scan, seven received a final diagnosis of “definite IE”, one of “possible IE” and two of “IE rejected”. Among the 17 patients with a negative PET/CT scan, four were false-negative and received a final diagnosis of definite IE. These patients underwent PET/CT after having started antibiotic therapy (≥48 h) or had a technically suboptimal examination.
Conclusion
In patients with a cardiac device, PET/CT increases the diagnostic accuracy of the modified Duke criteria for IE, particularly in the subset of patients with possible IE in whom it may help the clinician manage a challenging situation.



Similar content being viewed by others


References
Baddour LM, Bettmann MA, Bolger AF, Epstein AE, Ferrieri P, Gerber MA, et al. Nonvalvular cardiovascular device-related infection. Circulation. 2003;108:2015–31.
Cabell CH, Heidenreich PA, Chu VH, Moore CM, Stryjewski ME, Corey GR, et al. Increasing rates of cardiac device infection among Medicare beneficiaries: 1990-1999. Am Heart J. 2004;147:582–6.
Greenspon AJ, Patel JD, Lau E, Ochoa JA, Frisch DR, Ho RT, et al. 16-year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States 1993 to 2008. J Am Coll Cardiol. 2011;58:1001–6.
Baddour LM. Cardiac device infection – or not. Circulation. 2010;121:1686–7.
Li JS, Sexton DJ, Mick N, Nettles R, Fowler Jr VG, Ryan T, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30(4):633–8.
Habib G, Hoen B, Tornos P, Thuny F, Prendergast B, Vilacosta I, et al.; ESC Committee for Practice Guidelines (CPG). Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J. 2009;30:2369–413.
Habib G, Badano L, Tribouilloy C, Vilacosta I, Zamorano JL, Galderisi M, et al. Recommendations for the practice of echocardiography in infective endocarditis. Eur J Echocardiogr. 2010;11(2):202–19.
Evangelista A, Gonzalez-Alujas MT. Echocardiography in infective endocarditis. Heart. 2004;90:614–7.
Vilacosta I, Sarriai C, San Romran JA, Jimenez J, Castillo JA, Iturralde E, et al. Usefulness of transesophageal echocardiography for diagnosis of infected transvenous permanent pacemakers. Circulation. 1994;89:2684–7.
Lo R, D’Anca M, Cohen T, Kerwin T. Incidence and prognosis of pacemaker lead-associated masses: a study of 1,569 transesophageal echocardiograms. J Invasive Cardiol. 2006;18:599–601.
Victor F, De Place C, Camus C, Le Breton H, Leclercq C, Pavin D, et al. Pacemaker lead infection: echocardiographic features, management, and outcome. Heart. 1999;81:82–7.
Viganego F, O’Donoghue S, Eldadah Z, Shah MH, Rastogi M, Mazel JA, et al. Effect of early diagnosis and treatment with percutaneous lead extraction on survival in patients with cardiac device infection. Am J Cardiol. 2012;109:1466–71.
Sohail MR, Uslan DZ, Khan AH, Friedman PA, Hayes DL, Wilson WR, et al. Infective endocarditis complicating permanent pacemaker and implantable cardioverter-defibrillator infection. Mayo Clin Proc. 2008;83(1):46–53.
Kostakoglu L, Hardoff R, Mirtcheva R, Goldsmith S. PET-CT fusion imaging in differentiating physiologic from pathologic FDG uptake. Radiographics. 2004;24:1411–31.
Bertagna F, Bisleri G, Motta F, Merli G, Cossalter E, Lucchini S, et al. Possible role of F18-FDG-PET/CT in the diagnosis of endocarditis: preliminary evidence from a review of the literature. Int J Cardiovasc Imaging. 2012;28:1417–25.
Thuny F, Gaubert JY, Jacquier A, Tessonnier L, Cammilleri S, Raoult D, et al. Imaging investigation in infective endocarditis: current approach and prospectives. Arch Cardiovasc Dis. 2013;106:52–62.
Millar BC, Prandegrast BD, Alavi A, Moore JE. 18FDG-positron emission tomography (PET) has a role to play in the diagnosis and therapy of infective endocarditis and cardiac device infection. Int J Cardiol. 2013;167(5):1724–36.
Bonfiglioli R, Nanni C, Morigi JJ, Graziosi M, Trapani F, Bartoletti M, et al. 18F-FDG PET/CT diagnosis of ubexpected extracardiac septic embolism in patients with suspected cardiac endocarditis. Eur J Nucl Med Mol Imaging. 2013;40:1190–6.
Van Riet J, Hill EE, Gheysens O, Dymarkowski S, Herregods MC, Herijgers P, et al. 18F-FDG PET/CT for early detection of embolism and metastatic infection in patients with infective endocarditis. Eur J Nucl Med Mol Imaging. 2010;37:1189–97.
Ozcan C, Asmar A, Gill S, Thomassen A, Diederichsen ACP. The value of FDG-PET/CT in the diagnostic work-up of extra cardiac infectious manifestation in infectious endocarditis. Int J Cardiovasc Imaging. 2013;29:1629–37.
Sarrazin JF, Philippon F, Tessier M, Guimond J, Molin F, Champagne J, et al. Usefulness of fluorine-18 positron emission tomography/computed tomography for identification of cardiovascular implantable electronic device infections. J Am Coll Cardiol. 2012;59:1616–25.
Bensimhon L, Lavergne T, Hugonne F, Mainardi JL, Latremouille C, Maunoury C, et al. Whole body 18Ffluorodeoxyglucose positron emission tomography imaging for the diagnosis of pacemaker or implantable cardioverter defibrillator infection: a preliminary prospective study. Clin Microbiol Infect. 2011;17:836–44.
Ploux S, Riviere A, Amraoui S, Whinnett Z, Barandon L, Lafitte S, et al. Positron emission tomography in patients with suspected pacing system infections may play a critical role in difficult cases. Heart Rhythm. 2011;8:1478–81.
Amraoui S, Texier-Maugein J, Bordachar P. PET scan in suspected but unproven pacemaker endocarditis. Arch Cardiovasc Dis. 2012;105:125–6.
Kumar R, Basu S, Torigian D, Anand V, Zhuang H, Alavi A. Role of modern imaging techniques for diagnosis of infection in the era of 18F-fluorodeoxyglucose positron emission tomography. Clin Microbiol Rev. 2008;21(1):209–24.
Balink H, Hut E, Pol T, Flokstra FJ, Roef M. Suppression of 18F-FDG myocardial uptake using a fat-allowed, carbohydrate-restricted diet. J Nucl Med Technol. 2011;39:185–9.
Sohail MR, Uslan DZ, Khan AH, Friedman PA, Hayes DL, Wilson WR, et al. Management and outcome of permanent pacemaker and implantable cardioverter-defibrillator infections. J Am Coll Cardiol. 2007;49(18):1851–9.
Baddour LM, Epstein AE, Erickson CC, Knight BP, Levison ME, Lockhart PB, et al. Update on cardiovascular implantable electronic device infections and their management: a scientific statement from the American Heart Association. Circulation. 2010;121(3):458–77.
Wilkoff BL, Love CJ, Byrd CL, Bongiorni MG, Carrillo R, Crossely GH, et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: this document was endorsed by the American Heart Association (AHA). Heart Rhythm. 2009;6(7):1085–104.
Athan E, Chu V, Tattevin P, Selton-Suty C, Jones P, Naber C, et al. Clinical characteristics and outcome of infective endocarditis involving implantable cardiac devices. JAMA. 2012;307(16):1727–35.
Bongiorni MG, Tascini C, Tagliaferri E, Di Cori A, Soldati E, Leonildi A, et al. Microbiology of cardiac implantable electronic device infection. Europace. 2012;14:1334–9.
Kouijzer IJE, Vos FJ, Janssen JR, van Dijk APJ, Oyen WJG, Bleeker-Rovers CP. The value of 18F-FDG PET/CT in diagnosing infectious endocarditis. Eur J Nucl Med Mol Imaging. 2013;40(7):1102–7.
Treglia G, Bertagna F. Factors influencing the sensitivity of 18F-FDG PET/CT in the detection of infective endocarditis. Eur Nucl Med Mol Imaging. 2013;40:1112–3.
Kouijzer IJ, Vos FJ, Janssen MJ, van Dijk AP, Bleeker-Rovers CP, Oyen WJ. Reply to comment by Treglia and Bertagna: FDG PET/CT for detection of infectious endocarditis. Eur J Nucl Med Mol Imaging. 2013;40:1114–5.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Graziosi, M., Nanni, C., Lorenzini, M. et al. Role of 18F-FDG PET/CT in the diagnosis of infective endocarditis in patients with an implanted cardiac device: a prospective study. Eur J Nucl Med Mol Imaging 41, 1617–1623 (2014). https://doi.org/10.1007/s00259-014-2773-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-014-2773-z