
Abstract
Objective
The purpose of our study was twofold: to better understand the relationship between medial meniscal extrusion (MME) and degenerative joint disease (DJD), and to determine whether a relationship exists between MME and medial meniscal root (MMR) pathology, radial tear and joint effusion.
Design and patients
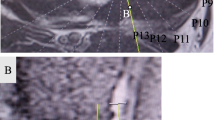
Two hundred and five consecutive MR imaging examinations of the knee were prospectively evaluated, regardless of indication, for the presence and degree of MME, medial compartment marginal osteophytes, medial compartment articular cartilage loss, joint effusion, medial meniscal tear and MMR pathology. MME ≥3 mm was considered abnormal. All studies were performed using a 1.5 T GE Signa MR unit with a quadrature knee coil. The standard protocol included oblique sagittal, coronal and axial imaging.
Results
We found a strong association (P<0.0001) between ≥3 mm MME and medial joint line osteophytosis (77%), medial compartment articular cartilage loss (69%), MMR pathology (64%) and radial tear (58%) when compared with knees without these findings. Fifty-one percent of cases with a moderate/large joint effusion had <3 mm MME. We found that 20% (31/155) of patients with minimal or no evidence of DJD had ≥3 mm MME. Of this group, 62% (19/31) had either MMR pathology and/or radial tear, 13% (4/31) had joint effusion as their only abnormality and 6% (2/31) had a normal examination (other than the presence of MME). The remaining 19% consisted of three cases of different types of meniscal tear and three cases of small joint effusions but no other detectable pathology.
Conclusion
MME ≥3 mm is strongly associated with DJD, MMR pathology and radial tear. A significant number of cases with no or minimal evidence of DJD (20%) had ≥3 mm MME, suggesting that MME precedes, rather than follows, the development of DJD. We also found that joint effusion was not strongly associated with ≥3 mm MME.





Similar content being viewed by others


References
Aagaard H, Verdonk R. Function of the normal meniscus and consequences of meniscal resection. Scand J Med Sci Sports 1999; 9:134–140.
Breitenseher MJ, Trattnig S, Dobrocky I, et al. MR imaging of meniscal subluxation in the knee. Acta Radiol 1997; 38:876–879.
Adams JG, McAlindon T, Dimasi M, Carey J, Eustace S. Contribution of meniscal extrusion and cartilage loss to joint space narrowing in osteoarthritis. Clin Radiol 1999; 54:502–506.
Miller TT, Staron RB, Feldman F, Cepel E. Meniscal position on routine MR imaging of the knee. Skeletal Radiol 1997; 26:424–427.
Seedhorn BB, Hargreaves DJ. Transmission of the load in the knee joint with special reference to the role of the menisci: part II. Eng Med 1979; 8:220–228.
Walker PS, Erkman MJ. The role of the menisci in force transmission across the knee. Clin Orthop 1975; 109:184–192.
Fairbank TJ. Knee joint changes after meniscectomy. J Bone Joint Surg 1948; 30B:664–670
Kenny C. Radial displacement of the medial meniscus and Fairbank’s signs. Clin Orthop 1997; 339:163–173.
Pagnani MJ, Cooper DE, Warren RF. Extrusion of the medial meniscus. Arthrosc J Arthrosc Rel Surg 1991; 7:297–300.
Author information
Authors and Affiliations
Corresponding author
Additional information
This paper was presented at the 2003 ARRS meeting
Rights and permissions
About this article
Cite this article
Lerer, D.B., Umans, H.R., Hu, M.X. et al. The role of meniscal root pathology and radial meniscal tear in medial meniscal extrusion. Skeletal Radiol 33, 569–574 (2004). https://doi.org/10.1007/s00256-004-0761-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-004-0761-2