
Abstract
Coronavirus disease of 2019 (COVID-19) is a cause of significant morbidity and mortality worldwide. Although COVID-19 clinical manifestations are mainly respiratory, major cardiac complications are being reported. The mechanism of cardiac injury and arrhythmias is unclear. Also, drugs currently used to treat the COVID-19 may prolong the QT interval and may have a proarrhythmic propensity. The study aims to investigate the effects of COVID-19 infection with asymptomatic and mild symptoms on trans-myocardial repolarization parameters in children without treatment. A total of 105 COVID-19 patients were compared with 40 healthy children. The patient and control group data were compared by calculating the QT interval, corrected QT (QTc), QT dispersion (QTd), QTc dispersion (QTcd), Tp-e, Tp-e dispersion, Tp-e/QT ratio, and Tp-e/QTc ratio on the 12-lead surface electrocardiogram. The mean age was determined as 11.2 ± 0.3 years in the patient group, and 10.8 ± 2.1 years in the control group. In the COVID-19 group, QTd, QTcd, Tp-e, Tp-e dispersion, Tp-e/QT ratio and Tp-e/QTc ratio were statistically higher than the control group. The ventricular repolarization was impaired even in asymptomatic children with COVID-19 infection. These results suggest the need to further assess the long terms risks of prolonged QT dispersion in the setting of COVID-19 infection.
Similar content being viewed by others

Introduction
A novel coronavirus, now designated SARS-CoV-2 (COVID-19), was identified as the cause of an outbreak of acute respiratory illness in Wuhan, a city in the Hubei Province of China [1]. Presentations of COVID-19 infection have ranged from asymptomatic/mild symptoms to severe illness. COVID-19 infection appears to be milder in children than in adults, although severe cases have been reported [2]. Acute myocardial damage, arrhythmia, and cardiogenic shock have been demonstrated in adult COVID-19 infection. Arrhythmias may be the first clinical sign of COVID-19 infection. Besides drugs such as hydroxychloroquine (HCQ) and azithromycin which are used to treat the disease may increase the risk of arrhythmia [3]. Therefore, these patients may have a higher risk of cardiac arrhythmias. The study aims to investigate the effects of COVID-19 infection with asymptomatic and mild symptoms on trans-myocardial repolarization parameters in children without treatment.
Materials and Methods
Patient Population
This prospective, cross-sectional, controlled, double-blind study was performed between April 2020 and May 2020 in the department of pediatric cardiology clinic of our hospital. This study was granted ethical approval by the local clinical research ethics committee of our hospital. All parents gave informed consent for participation in the study. The study included 105 children with COVID-19 infection and 40 children age- and sex-matched healthy subjects with an innocent murmur as a control group. The children included the study subjected to full history-taking, and complete physical examination was performed. Heart rate and blood pressure of all children were recorded. Exclusion criteria consisted of signs of heart failure except for tachycardia increased cardiac enzymes, pathology except for sinus tachycardia in electrocardiography (ECG), cardiomegaly on chest X-Ray and treated with HCQ/azithromycin. Also, children with the structural and functional cardiac abnormality, any other systemic disorders, and comorbid diseases were excluded. We did not routinely perform echocardiography on our patients due to the risk of transmission. The severity of the disease was classified as asymptomatic, mild, moderate, severe and critical according to the symptoms and signs of the patients with positive 2019-nCoV nucleic acid test results. The patients with no signs or symptoms were defined as “asymptomatic”. The patients with symptoms of acute upper respiratory tract infection such as fever, fatigue, muscle pain, headache, loss of sense of smell, red-eye, cough, sore throat, runny nose and sneezing, and digestive symptoms such as nausea, vomiting, abdominal pain and diarrhea were classified as “mild”. Presence of pneumonia, fever, frequent cough but with no obvious hypoxemi were defined as “moderate”. Presence of dyspnea with central cyanosis, oxygen saturation < 92% with other hypoxia manifestations were defined as “severe”. Presence of acute respiratory distress syndrome (ARDS), respiratory failure, shock, encephalopathy, myocardial injury, heart failure, coagulation dysfunction, and organ dysfunction were defined as “critical”.
Electrocardiography
All ECGs at the time of diagnosis of COVID-19 infection were analyzed from the medical records of the patients. We examined 12-lead ECG recordings at a speed of 25 mm/s and amplitude of 10 mm/mV with the patient lying down. During the ECG recording, all the children were in sinus rhythm. The high-resolution computer software program (Adobe Photoshop CS2) was used for the evaluation of ECG results by a single observer. The QRS interval was measured from the start of the Q-wave or in absence of the Q-wave, from the start of the R-wave to the end of S, that is, to its return to the isoelectric line. The measurement of the QT interval was started from the onset of the QRS complex until the end of the T-wave. A discrete U-wave after T- wave was excluded from measurement. In the case of the fusion of two waves, the U component was included. The biphasic T-wave was defined as the T-wave with equal and opposite amplitude. When this occurred the point at which the last part of the wave crossed the isoelectric line was taken into account. QT and QTc dispersion was calculated as the difference between the maximum and minimum QT and QTc duration. The QTc duration was calculated using Bazett’s formula [4]. Measuring from the peak of the T-wave to the end of the T-wave provided the Tp-e interval, which was defined as the intersection of the isoelectric line with the tangent to the downslope of the T-wave in precordial leads [5]. The Tp-e duration was calculated by measuring the distance between the two points in the isoelectric line. The difference between the maximum and the minimum Tp-e in the precordial leads was the Tp-e dispersion. Based on these measurements, Tp-e, Tp-e dispersion and Tp-e/QT ratio were calculated.
Statistical Analysis
The statistical package SPSS version 11.5 (SPSS Inc., Chicago, IL, USA) was used for data analysis. Descriptive statistics are presented as mean ± SD. Pearson and Chi-square analyses were used to compare frequencies of findings. Independent samples Student t test was used to compare continuous variables in the obese group and the control group. A p value <0.05 was considered statistically significant.
Results
The mean age was determined as 11.2 ± 0 .3 years (median 12.9 years, range 2 months-18 years) in the patient group, and 10.8 ± 2.1 years (median 11.6 years, range 5 months − 16 years) in the control group. 61.8% of the patients (n = 65) were diagnosed between the ages of 10–18 years. No statistically significant difference was determined between the patient and control groups in respect of age, gender, and blood pressure values. The heart rate was higher in patient group. According to the clinical parameters, we found 51.4% of cases to be asymptomatic and 48.5% of cases to be mild. None of the patients to be in the moderate, severe and critical cases during their illness. Also noted the cardiac Troponin I, creatine kinase-myocardial band (CK-MB) and D-dimer values were normal ranges in our patients with COVID-19 infection. A pulse oximeter can measure normal oxygen saturation levels in our cases. Mean WBC, neutrophil, lymphocyte, and hemogram was normal. WBC was normal (3.9–10.2 × 109/L) in eighty four cases (84/105, 80.1%), decreased (< 3.9 × 109/L) in twelve cases (12/105, 11.4%), and increased (> 10.2 × 109/L) in nine cases (9/105, 8.5%).CRP increased in 32 cases (32/105, 30.4%), noted within their laboratory findings: mean CRP 9.9 ± 18.2 (1.8–133) mg/L. The demographic, clinical, and laboratory characteristics of both groups are shown in Table 1.
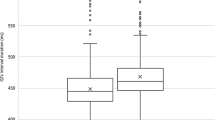
Baseline electrocardiograms were non-specific in a patient group except sinus tachycardia. The minimum QT and QTc minimum durations were found to be similar in the two groups (p > 0.05). The duration of QT dispersion was found to be significantly longer in the patient group (45.30 ± 6.1) than in the control group (27.11 ± 7.2; p < 0.01). QTc dispersion duration was found to be significantly increased in the patient group (36.30 ± 14.7) compared with the control group (14.5 ± 10.6; p < 0.01). Tpeak–end, Tpeak–end dispersion value, T peak–end/QT and T peak–end/QTc ratio in the patient group was significantly higher than control group. The QTmin, QTmax, QTcmin, QTcmax, QTd, QTcd, Tp-e, Tp-e dispersion, Tp-e/QT, and Tp-e/QTc ratio values of both groups are shown in Table 2.
Discussion
In December 2019, a novel coronavirus was identified as the cause of a cluster of pneumonia cases in Wuhan, a city in the Hubei province of China. It spreads rapidly around the World and the World Health Organization declared COVID-19 a pandemic on March 11, 2020 [1, 6]. The symptoms of COVID-19 are similar in children and adults. Fever and cough are the most common reported symptoms in children [7]. But COVID-19 appears to be milder in children than in adults. Sinus tachycardia caused by hypoxia and fever is common in the course of the disease. Although COVID-19 clinical manifestations are mainly respiratory, acute myocardial damage, arrhythmia and cardiogenic shock have been observed in adult COVID-19 infection. Acute myocarditis, as well as ventricular arrhythmias, might represent the first clinical manifestation of COVID-19 infection [8, 9]. Also, some drugs currently used to treat the COVID-19 are known to prolong the QT interval and can have a proarrhythmic propensity [3].
We investigated dispersion analysis in children with COVID-19 in comparison with those of age- and gender-matched control subjects. In the current study, QTd, QTcd, Tp-e dispersion and Tp-e/QT and Tp-e/QTc ratio were detected to be significantly greater in patients with COVID-19 than in the control subjects.
The T-wave is indicative of ventricular repolarization. It has been reported that trans-myocardial repolarization parameters, which include Tp-e, Tp-e dispersion, QT interval, QTc, QTc dispersion and the Tp-e/QT ratio, are associated with an increased risk of cardiac arrhythmia [10,11,12]. The normal range for QT and QTc dispersion are 40–50 ms and 10–44 ms in adults, respectively [13, 14]. In a review, Malik et al. [15] researched 51 studies in which QT dispersion was measured in 56 groups with a total of 8.455 healthy subjects including three studies of healthy children, and they showed that reported values of QT dispersion vary widely range from 10.5 to 71 ms. However, sharp limits for the QT and QTc interval dispersion are not seen for the pediatric age in the literature. Tutar et al. [16] found QTd and QTcd on average 29.9 and 47.3 ms, respectively in 174 pediatric children with a mean age of 12 years. Similar to our study, in a paper studying QT dispersion in pediatric cases with subclinical hypothyroid, QT and QTc dispersion in the control group were found to be 18.5 and 39.8, respectively [17]. In a large healthy adult population (n = 1555), Macfarlane et al. [18] reported that the upper limit of QT dispersion was 40 ms. QT dispersion > 40 ms was found to have 88% sensitivity and 57% specificity for prediction of the inducibility of sustained VT during an another electrophysiology study [19]. In our study, QT and QTc dispersion were found as 45.30 ± 6.1 and 36.30 ± 14.7 ms, respectively, and they were statistically higher than the control group.
The mechanism of cardiac injury and triggering arrhythmias is unclear but the severe systemic and myocardial inflammatory reaction seems to be one of the most plausible. Other proposed mechanisms of myocardial injury might be related to ACE2 [20]. There are few published studies about cardiac complications with COVID- 19 patients. They observed that acute cardiac injury, shock, and arrhythmias were present in 7.2%, 8.7%, and 16.7% of patients, respectively. Arrhythmias are common in adult patients with COVID-19 [8, 21, 22]. In another study, Hui et al. [23] reported ECG findings in 17/41 patients, of whom three had tachycardia with a higher prevalence in severe and critical cases. Guo et al. [24] reported ventricular tachycardia/ventricular fibrillation in 5.9% of patients with COVID-19 infection. In our study, no ventricular arrhythmia was recorded.
Another essential aspect to be discussed is about drugs causing prolongation of qt interval since these drugs (e.g. HCQ and azithromycin) recommended in the treatment of pediatric COVID-19 infection. These drugs can induce QT interval prolongation, an extremely rare but potentially fatal side effect, due to the risk of induced polymorphic ventricular tachycardia [25,26,27]. Close monitoring of the patient is required during the initiation and follow-up of these drugs, which can lead to prolonged QT intervals. In our study, we did not use these drugs in our patients.
Conclusion
We conclude that the ventricular repolarization was impaired even in asymptomatic children with COVID-19 infection. The risk of development of ventricular arrhythmia might be increased in COVID-19 patients. A baseline ECG should be performed in all COVID-19 positive children especially planned to receive QT prolonging medications along with serial monitoring. The patients with COVID-19 have a change in repolarization characteristics but may be still in normal range; thus, caution should be taken when prescribing QT prolonging medications.
References
Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese center for disease Control and prevention. J Am Med Assoc
Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, Tong S (2020) Epidemiology of COVID-19 among children in China. Pediatrics
Zheng Y-Y, Ma Y-T, Zhang J-Y, Xie X (2020) COVID-19 and the cardiovascular system. Nat Rev Cardiol
Bazett HC (1920) The time relations of the blood-pressure changes after excision of the adrenal glands, with some observations on blood volume changes. J Physiol 53:320–39
Gupta P, Patel C, Patel H, Narayanaswamy S, Malhotra B, Green JT et al (2008) T(p-e)/QT ratio as an index of arrhythmogenesis. J Electrocardiol 41:567–574
World Health Organization (WHO) (2020) WHO Director-General's opening remarks at the media briefing on COVID-19. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020.
Bialek S, Gierke R, Hughes M, McNamara L, Pilishvili T, Skoff T (2020) Coronavirus disease 2019 in children - United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep. 69(14):422–426
Hu H, Ma F, Wei X, Fang Y (2020) Coronavirus fulminant myocarditis saved with glucocorticoid and human immunoglobulin. Eur Heart J. https://doi.org/10.1093/eurheartj/ehaa190
Inciardi RM, Lupi L, Zaccone G et al (2020) Cardiac involvement in a patient with coronavirus disease 2019 (COVID-19). JAMA Cardiol. https://doi.org/10.1001/jamacardio.2020.1096
Castro Hevia J, Antzelevitch C, TornesBarzaga F, Dorantes Sanchez M, Dorticos Balea F, Zayas Molina R et al (2006) Tpeak-Tend and Tpeak-Tend dispersion as risk factors for ventricular tachycardia/ventricular fibrillation in patients with the Brugada syndrome. J Am Coll Cardiol 47:1828–1834
Hlaing T, Guo D, Zhao X, DiMino T, Greenspon L, Kowey PR et al (2005) QT and Tp-e intervals in left and right chest leads: comparison between patients with systemic and pulmonary hypertension. J Electrocardiol 38:154–158
Ozyurt A, Karpuz D, Yucel A, Tosun M, Kibar AE, Hallioglu O (2017) Effects of acute carbon monoxide poisoning on ECG and echocardiographic parameters in children. Cardiovasc Toxicol 17:326–334
Van de Loo A, Arendts W, Hohnloser SH (1994) Variability of QT dispersion measurements in the surface electrocardiogram in patients withacute myocardialinfarction and in normal subjects. Am J Cardiol 74:1113–8
Macfarlane PW, McLaughlin SC, Rodger JC (1998) Influence of lead selection andpopulation on automated measurement of QT dispersion. Circulation 98:2160–7
Malik M, Batchvarov VN (2000) Measurement, interpretation and clinical potential of QT dispersion. J Am Coll Cardiol 36:1749–1766
Tutar HE, Öcal B, Imamoglu A, Atalay S (1998) Dispersion of QT and QTc interval in healthy children, and effects of sinus arrhythmia on QT dispersion. Heart 80:77–79
Akın A, Unal E, Yıldırım R, Ture M, Balık H, Haspolat YK (2018) Evaluation of QT dispersion and Tp-e interval in children with subclinical hypothyroidism. Pac Clin Electrophysiol 41:372–375
Macfarlane PW, McLaughlin SC, Yang TF (1994) EVects of age, sex, and race on ECG interval measurements. J Electrocardiol 27:14–19
Goldner B, BrandspiegelHZ HL, Jadonath R, Jadonath TJ (1995) Utility of QT dispersion combined with the signal-averaged electrocardiogram in detecting patients susceptible to ventricular tachyarrhythmia. Am J Cardiol 76:1192–1194
Zhu H, Rhee JW, Cheng P, Waliany S, Chang A, Witteles RM, Maecker H, Davis MM, Nguyen PK, Wu SM (2020) Cardiovascular complications in patients with COVID-19: consequences of viral toxicities and host immune response. Curr Cardiol Rep 22(5):32. https://doi.org/10.1007/s11886-020-01292-3
Shi S, Qin M, Shen B et al (2020) Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA. https://doi.org/10.1001/jamacardio.2020.0950
Wang D, Hu B, Hu C et al (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. https://doi.org/10.1001/jama.2020.1585
Hui H, Zhang Y, Yang X et al (2020) Clinical and radiographic features of cardiac injury in patients with 2019 novel coronavirus pneumonia. MedRxiv. https://doi.org/10.1101/2020.02.24.20027052
Guo T, Fan Y, Chen M et al (2020) Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. https://doi.org/10.1001/jamacardio.2020.1017
Seshadri MS, John L, Varkey K, Koshy TS (1979) Ventricular tachycardia in a patient on dehydroemetine and chloroquine for amoebic liver abscess. Med J Aust 1:406–7
Fauchier JP, Fauchier L, Babuty D, Breuillac JC, Cosnay P, Rouesnel P (1993) Druginduced ventricular tachycardia. Arch Mal Coeur Vaiss 86:757–67
Siqueira-Batista R, Ramos Júnior AN, Pessanha BS, Sforza-de-Almeida MP, Potsch DF (1998) Chloroquine and cardiac arrhythmia: case report. East Afr Med J 75:117–9
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ece, İ., Koçoğlu, M., Kavurt, A.V. et al. Assessment of Cardiac Arrhythmic Risk in Children With Covid-19 Infection. Pediatr Cardiol 42, 264–268 (2021). https://doi.org/10.1007/s00246-020-02474-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-020-02474-0