
Abstract
Purpose
This study aimed to conduct a multivariate analysis to identify independent factors that predict tibial tunnel widening (TW) after anatomical anterior cruciate ligament (ACL) reconstruction using bone–patellar tendon–bone (BPTB) grafts.
Methods
In total, 103 patients who underwent ACL reconstructions using BPTB grafts were included. Tunnel aperture area was measured using three-dimensional computed tomography 1 week and 1 year postoperatively, and the tibial TW was calculated. The patients were divided into group S comprising 58 patients who had tibial TW < 30% and group L comprising 45 patients who had tibial TW > 30%, retrospectively. Using univariate analyses, age, gender, body mass index, Tegner activity scale, the time between injury and surgery, tibial tunnel location, tibial tunnel angle, medial posterior tibial slope, lateral posterior tibial slope, and length of the tendon in the tibial tunnel were compared between two groups. Multivariate regression analysis was conducted to reveal the independent risk factors for the tibial TW among preoperative demographic factors and radiographic parameters that correlated with the tibial TW in the univariate analyses.
Results
Compared with those at 1 week postoperatively, mean tibial tunnel aperture areas were increased by 30.3% ± 26.8% when measured at 1 year postoperatively. The lateral posterior tibial slope was significantly larger (p < 0.001), and the length of the tendon within the tibial tunnel was significantly longer in group L than that in group S (p = 0.03) in the univariate analyses. Multivariate regression analysis showed that the increase in lateral posterior tibial slope (p = 0.001) and the length of the tendon within the tibial tunnel (p = 0.03) were predictors of the tibial TW.
Conclusions
This study showed that increased lateral posterior tibial slope and a longer tendinous portion within the tibial tunnel were independent factors that predicted the tibial TW following anatomical ACL reconstruction with a BPTB graft.
Level of evidence
III.
Similar content being viewed by others

Introduction
Tunnel widening (TW) after anterior cruciate ligament (ACL) reconstruction is a well-known phenomenon. The presence of expanded tunnels often severely complicates revision ACL reconstruction and sometimes requires staged surgery, and it could delay the return to daily living activities and sport [21, 35, 36]. The interplay between biological and mechanical factors is known to be responsible for TW. The biological factors include joint fluid access between the graft and the bone that contains osteolytic cytokines [4]. Mechanical factors include the bony morphology, improper tunnel position, excessive initial graft tension, graft motion within the tunnel, and accelerated rehabilitation [2, 11, 17, 20, 21, 29]. Moreover, the role of the posterior tibial slope (PTS) on the ACL injury mechanism [6, 10, 19, 34], grade 3 pivot shift [26], graft failure [9, 13, 15, 39, 40], and TW [14, 17, 21] has been discussed in previous literature.
More recent approaches to anatomical ACL reconstruction include the use of BPTB grafts, with a newly developed rectangular tunneling technique [24]. The distal end of the femoral bone plug is typically positioned to match the femoral tunnel aperture; therefore, the location of a bone plug in the tibial tunnel is naturally determined, and the tibial TW is concerned. Taketomi et al. have reported that the length of the tendon within the tibial tunnel affected the tibial TW following anatomical ACL reconstruction using a BPTB graft [27]. However, the causes of the tibial TW may be multifactorial, and several other factors may affect the tibial TW, such as age, tunnel location, tunnel angle, or the posterior slope of the tibia [11, 17, 18, 21, 38]. Most previous studies that examined factors affecting the tibial TW included ACL reconstruction with a hamstring graft or only conducted a univariate analysis. This study aimed to identify the independent factors that affect the tibial TW after anatomical ACL reconstruction using a BPTB graft.
Material and methods
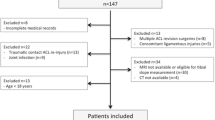
The institutional review board of the University of Tokyo approved this retrospective study (approval no. 2674). Patients and their families were informed that data from their cases would be submitted for publication; all included patients provided written informed consent. Using a BPTB graft at our institute between 2013 and 2017, a total of 154 consecutive patients underwent ACL reconstruction. Of these, 103 patients were included in the present study. The exclusion criteria were (1) previous intra-articular ligament reconstruction; (2) previous osteotomy around the knee joint; and (3) the presence of posterior cruciate ligament insufficiency, abnormal varus/valgus instability, or concomitant reconstruction of other ligaments. In total, 20 patients were excluded, that is, 10, 4, and 6 corresponding to the first, second, and third exclusion criteria, respectively. Additionally, 3 patients suffered reinjury before the end of the follow-up period 1 year postoperatively, and 15 patients were lost to follow-up (11.2% dropout). Thirteen patients were excluded because postoperative three-dimensional computed tomography (3-D CT) scans were not available. An experienced surgeon participated in all procedures as either an operator or the first assistant. Our final analysis involved 29 females and 74 males with a median age of 27 years (range, 15–58 years). According to the average tibial TW in the present study, the patients were divided into two groups, namely, group S (n = 58; tibial TW < 30%) and group L (n = 45; tibial TW ≥ 30%). Table 1 summarizes the preoperative patient information.
Surgical procedure
The autologous BPTB grafts were harvested from the central portion of the patellar tendon that were 10 mm wide and had bone plugs at either end [28]. As described by Shino et al., the femoral bone plug for a rectangular tunnel was usually 6 × 10 × 15 mm [24]. The femoral insertion site was determined after evaluating bony landmarks (i.e., the lateral intercondylar ridge and the lateral bifurcate ridge) [7, 25]. In creating the femoral tunnel, our priority was to position the femoral tunnel apertures as posteriorly and proximally as possible within the femoral footprint of the ACL [30]. A rectangular tunnel (6 × 10 mm) was created through a distal anteromedial portal. On the tibial side, a rectangular tunnel (6 × 10 mm) was created using the outside-in technique, and it was over-drilled halfway using a 10 mm cannulated drill bit. In creating the tibial tunnels, our priority was to position the tibial tunnel apertures as anteriorly and medially as possible within the tibial footprint of the ACL in reference to the ACL remnant, the medial tibial eminence, the anterior horn of the lateral meniscus, the intermeniscal ligament, and the posterior cruciate ligament [32, 33]. The femoral bone plug was connected to an EndoButton (Smith & Nephew Endoscopy, Andover, MA) using no. 5 FiberWire (Arthrex, Inc., Naples, FL) and no. 3 nonabsorbable sutures [28]. The tibial bone plug is typically a 10 mm diameter cylinder, and its length is approximately 15 mm. This plug was connected to a small double spike plate (Smith & Nephew Endoscopy) and a half-threaded 5.0 mm cancellous screw using no. 5 FiberWire and no. 5 nonabsorbable suture. This was fixed at full knee extension with an 80 N pull using a ligament tensioner (Smith & Nephew Endoscopy) [31].
Postoperative rehabilitation
Identical rehabilitation protocols were applied for all patients. In brief, the knee was not immobilized but was protected for 6 weeks using a functional brace. Immediately after the surgery, active and assisted range-of-motion exercises were commenced. Partial weight-bearing activity commenced 2 days postoperatively and full weight-bearing activity 1 week postoperatively. Patients were permitted to run 4 months postoperatively and were allowed to return to previous sporting activities at an average of 8–9 months postoperatively.
Radiographic evaluation
Standard anteroposterior and lateral radiographs of the knee obtained 1 week postoperatively were used to measure the angles between the tunnel and the tibial plateau. For all patients, 3-D CT scanning was conducted on the reconstructed knee 1 week and 1 year postoperatively using a helical high-speed Aquilion PRIME, Aquilion precision, or Aquilion ONE (Toshiba Medical Systems Co., Japan) CT machine. The ZIOSTATION software package (Ziosoft Inc., Tokyo, Japan) was used to create a 3-D reconstruction of the knee. For measuring the location of the tibial tunnel aperture, first, the 3-D model of the proximal tibia was realigned to obtain a true proximal-to-distal view. Thereafter, tibial anatomic coordinate axes were established on the image, as described by Forsythe et al. [8], and the center of the ellipse approximated to the tunnel aperture shape was determined. Finally, the anterior-to-posterior and medial-to-lateral positions were measured to evaluate aperture location (Fig. 1) [31]. The medial and lateral PTSs were measured using CT according to the previously reported method via magnetic resonance imaging [12]. The central sagittal CT slice was used to determine the longitudinal axis of the tibia. One circle was fitted to the proximal tibia, tangential to the cortexes, and a second circle was fitted distally with its center placed on the border of the first circle. The line connecting the center of these two circles was considered the longitudinal axis (Fig. 2A). Using a coronal view, the mid-sagittal images of the medial and lateral tibiofemoral compartments were selected. The medial and lateral PTS were determined using the angle between the axis perpendicular to the longitudinal axis and the line connecting the most proximal anterior and posterior subchondral bone points of the medial and lateral tibiofemoral compartments (Fig. 2B). Nagai et al. reported that the inter-rater intraclass correlation coefficient of PTS measurements using this method was 0.803, which was highly reliable [17]. For measuring the tendinous portion length within the tibial bone tunnel, after the long axes of the tibial tunnel view had been created via multiplanar reconstruction, the distance between the center of the tibial tunnel aperture and the center of the proximal end of the bone plug was measured on the bone tunnel’s central axis [27]. For TW evaluation, the aperture area was measured using the ImageJ software (National Institutes of Health, Bethesda, MD), calibrated to the CT image scale (Fig. 3) [22]. The tunnel aperture area was measured 1 week postoperatively as the baseline measurement, which was then compared with the diameter measured at the 1 year follow-up. Subsequently, the proportional variation in the tibial tunnel aperture area between the two points, defined as TW (%), was determined. All measurement methods allow one decimal, and the results were reported with one decimal. The two investigators (K.N. and S.T.) conducted the CT measurements. It was previously reported that the intraobserver and interobserver intraclass correlation coefficients of the tibial tunnel aperture area measurements using this method were 0.97 and 0.94, respectively [27]. The intraobserver and interobserver intraclass correlation coefficients for measurement of intra-tunnel tendon length were 0.97 and 0.95, respectively, in a randomly selected ten-case pilot study.

Evaluation of tibial tunnel location. The center of the ellipse approximated to the tunnel aperture shape was determined. Anterior-to-posterior positions (a) were calculated as a percentage of the distance from the line through the anterior border of the tibial plateau to the line running through the posterior border of the tibial plateau. Medial-to-lateral positions (m) were calculated as a percentage of the distance from the line through the medial border of the tibial plateau to the line running through the lateral border of the tibial plateau

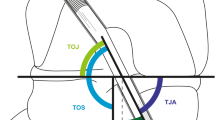
Measurements of posterior tibial slope (PTS) on CT images. The arrow indicates the angle of lateral PTS. CT computed tomography

Measurements of the tibial tunnel aperture area on 3-D CT. A true proximal-to-distal view of the proximal tibia (along with an appropriate scale bar) was downloaded onto a computer; using the ImageJ software (National Institutes of Health, Bethesda, MD, USA), calibrated to the scale of the CT image, the area of tibial tunnel aperture was manually traced and analyzed. 3-D three-dimensional, CT computed tomography
Statistical analysis
Statistical analysis was conducted using BellCurve for Excel (SSRI Co., Ltd., Tokyo, Japan). Patient parameters were compared using the unpaired two-tailed Student t test, the Mann–Whitney U test, and the Fisher exact test. Using the unpaired two-tailed Student t test, radiographic parameters were compared. Multivariate regression analysis was conducted to detect the factors that correlated significantly to the tibial TW among age, gender, BMI, and radiographic parameters found to correlate with the tibial TW in the univariate analyses. Pearson’s correlation analyses were conducted to evaluate the correlations between the detected factors in the multivariate analysis and the tibial TW. Statistical significance was set at p < 0.05. An a priori sample size calculation was conducted with G*Power Software 3.1.9.2. Ninety-two patients were required to achieve a power of 0.80, with an effect size f2 of 0.15 as moderate and an alpha of 0.05 [3].
Results
Compared with those at 1 week postoperatively, the mean tibial tunnel aperture areas were increased by 30.3% ± 26.8% when measured at 1 year postoperatively. No significant differences were observed between the two groups in terms of demographic data. Among radiographic parameters, lateral PTS in group L was significantly larger than that in group S (p < 0.001), and the length of the tendon within the tibial tunnel in group L was significantly longer than that in group S (p = 0.03). No significant differences were observed between other radiographic parameters and the tibial TW with the univariate analyses (Table 2). Using age, gender, BMI, lateral PTS, and the length of the tendon within the tibial tunnel, multivariate regression analysis was conducted. Multivariate analysis showed the lateral PTS (p = 0.001) and length of the tendon within the tibial tunnel (p = 0.03) were predictors of the tibial TW (Table 3). Figures 4 and 5 show the detailed data on the factors included in the multivariate analysis. Increase in lateral PTS (r = 0.34, p < 0.001) and the length of the tendon within the tibial tunnel (r = 0.29, p = 0.003) were significantly correlated with an increased tibial TW.

Correlation between the lateral posterior tibial slope (PTS) and tibial tunnel widening. The lateral PTS was positively correlated with tibial tunnel widening (r = 0.34, p < 0.001)

Correlation between the length of the tendon within the bone tunnel and tibial tunnel widening. The length of the tendon within the bone tunnel was positively correlated with tibial tunnel widening. (r = 0.29, p = 0.003)
Discussion
The most important findings of the present study were that multivariate analysis revealed an increased lateral PTS and a longer tendinous portion within the bone tunnel were independent factors that predicted the tibial TW following anatomical ACL reconstruction using a BPTB graft.
One previous study showed that the tibial TW correlated to lateral PTS after ACL reconstruction with a hamstring graft by measuring the tunnel diameter on standard plain radiographs [21]. It has also been shown that the tibial TW correlated with medial and lateral PTS after ACL reconstruction with a quadriceps tendon graft. This was conducted by calculating the tibial TW determined by dividing the cross-sectional area of the tibial tunnel using CT by the nominal area calculated according to the diameter of the tibial tunnel dilator during the surgery under univariate analyses [17]. Using a multivariate analysis, the present study revealed that the tibial TW was independently correlated to lateral PTS after anatomical rectangular tunnel ACL reconstruction using a BPTB graft by measuring TW on CT. An increased PTS can result in anterior translation of the tibia during weight-bearing activities, potentially placing more strain on the ACL resulting in increased ACL injury risk [1, 5, 16]. This mechanism may cause the tibial TW after ACL reconstruction.
Taketomi et al. reported that the longer tendinous portion within the tibial tunnel resulted in a greater tibial TW following anatomical ACL reconstructions using a BPTB graft [27]. However, in their study, the authors only targeted the length of the tendon within the bone tunnel. Another previous report demonstrated that the longer tendinous portion within the tibial tunnel was a factor related to the tibial TW [18]. Nevertheless, the sample size of that study was relatively small. The length of the tendon within the tibial tunnel, tunnel location, and tunnel angle has been regarded to be related to one another. Thus, further investigation using a multivariate regression analysis of such factors was conducted to elucidate independent factors that affect the tibial TW. Consequently, in the present study, we investigated such factors in a larger cohort using a multivariate regression analysis and found that the length of the tendon within the tibial tunnel was detected to be one of the independent factors that affect the tibial TW.
In the present study, no significant difference was observed between the two groups in terms of tunnel location, whereas in previous reports, it has been demonstrated that the tunnel location affected the tibial TW [23, 37]. In the present study, tunnel location showed small variations because of anatomical concepts used for tunnel placement, and this might be the reason why tunnel location did not affect the tibial TW. Regarding age, no significant difference was observed between the two groups in the present study. A correlation between age and TW after ACL reconstruction was reported using a hamstring tendon graft [38]; however, this correlation may not be applicable for BPTB grafts.
The intraoperative tendon length adjustment within the tibial tunnel is challenging because the distal end of the femoral bone plug is typically positioned to match the femoral tunnel aperture and the location of the bone plug in the tibial tunnel is naturally determined [27]. In terms of clinical relevance, our results suggest that the lateral PTS and the length of the tendon within the tibial tunnel should be postoperatively measured. When managing large PTS or increased tendon length within the tibial tunnel, surgeons may avoid the tibial TW by considering more conservative physical therapy at an early stage following the surgery. The use of either additional rigid fixation on the tibial side or biological agents to accelerate bone–tendon healing could be alternative approaches.
There were several limitations in the present study. First, this was a retrospective study involving a relatively small cohort. Second, in this study, we only targeted the tibial TW and femoral TW might affect the tibial TW. Third, the effect of meniscus status on TW was not evaluated in this study. Fourth, the patients were divided into two groups according to the tibial TW based on its average in the present study, however, whether this cutoff value was appropriate was unclear. Moreover, another cutoff value may be required for ACL reconstruction using grafts that were fixed using different devices. Fifth, the present study did not analyze the effects of the tibial TW on clinical outcomes after ACL reconstruction. Sixth, CT images were only acquired at two time points (1 week and 1 year postoperatively). Thus, the tibial TW that occurred at any other time point may not have been detected. Finally, the follow-up period was relatively short. However, TW occurs primarily during the first 6 months after surgery and remains unchanged thereafter; hence, 1 year after surgery is an appropriate time to evaluate TW [35].
Conclusions
Increased lateral PTS and a longer tendinous portion within the bone tunnel were the independent factors that predicted the tibial TW following anatomical ACL reconstruction using a BPTB graft. Surgeons should be aware that the lateral PTS and length of the tendon within the tibial tunnel may affect the tibial TW after anatomical ACL reconstruction using a BPTB graft.
References
Bernhardson AS, Aman ZS, Dornan GJ, Kemler BR, Storaci HW, Brady AW, Nakama GY, LaPrade RF (2019) Tibial slope and its effect on force in anterior cruciate ligament grafts: anterior cruciate ligament force increases linearly as posterior tibial slope increases. Am J Sports Med 47(2):296–302
Choi NH, Lee SJ, Park SC, Victoroff BN (2020) Comparison of postoperative tunnel widening after hamstring anterior cruciate ligament reconstructions between anatomic and nonanatomic femoral tunnels. Arthroscopy 36(4):1105–1111
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associated, Hillsdale, pp 410–414
Darabos N, Haspl M, Moser C, Darabos A, Bartolek D, Groenemeyer D (2011) Intraarticular application of autologous conditioned serum (ACS) reduces bone tunnel widening after ACL reconstructive surgery in a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc 19(Suppl 1):S36–S46
Dejour D, Pungitore M, Valluy J, Nover L, Saffarini M, Demey G (2019) Tibial slope and medial meniscectomy significantly influence short-term knee laxity following ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 27(11):3481–3489
DePhillipo NN, Zeigler CG, Dekker TJ, Grantham WJ, Aman ZS, Kennedy MI, LaPrade RF (2019) Lateral posterior tibial slope in male and female athletes sustaining contact versus noncontact anterior cruciate ligament tears: a prospective study. Am J Sports Med 47(8):1825–1830
Ferretti M, Ekdahl M, Shen W, Fu FH (2007) Osseous landmarks of the femoral attachment of the anterior cruciate ligament: an anatomic study. Arthroscopy 23(11):1218–1225
Forsythe B, Kopf S, Wong AK, Martins CA, Anderst W, Tashman S, Fu FH (2010) The location of femoral and tibial tunnels in anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Joint Surg Am 92(6):1418–1426
Grassi A, Signorelli C, Urrizola F, Macchiarola L, Raggi F, Mosca M, Samuelsson K, Zaffagnini S (2019) Patients with failed anterior cruciate ligament reconstruction have an increased posterior lateral tibial plateau slope: a case-controlled study. Arthroscopy 35(4):1172–1182
Grassi A, Pizza N, Zambon Bertoja J, Macchiarola L, Lucidi GA, Dal Fabbro G, Zaffagnini S (2020) Higher risk of contralateral anterior cruciate ligament (ACL) injury within 2 yr after ACL reconstruction in under-18-year-old patients with steep tibial plateau slope. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06195-y
Höher J, Möller HD, Fu FH (1998) Bone tunnel enlargement after anterior cruciate ligament reconstruction: fact or fiction? Knee Surg Sports Traumatol Arthrosc 6(4):231–240
Hudek R, Schmutz S, Regenfelder F, Fuchs B, Koch PP (2009) Novel measurement technique of the tibial slope on conventional MRI. Clin Orthop Relat Res 467(8):2066–2072
Jaecker V, Drouven S, Naendrup JH, Kanakamedala AC, Pfeiffer T, Shafizadeh S (2018) Increased medial and lateral tibial posterior slopes are independent risk factors for graft failure following ACL reconstruction. Arch Orthop Trauma Surg 138(10):1423–1431
Ko YW, Rhee SJ, Kim IW, Yoo JD (2015) The correlation of tunnel position, orientation and tunnel enlargement in outside-in single-bundle anterior cruciate ligament reconstruction. Knee Surg Relat Res 27(4):247–254
Lee CC, Youm YS, Cho SD, Jung SH, Bae MH, Park SJ, Kim HW (2018) Does posterior tibial slope affect graft rupture following ACL reconstruction? Arthroscopy 34(7):2152–2155
Marouane H, Shirazi-Adl A, Adouni M, Hashemi J (2014) Steeper posterior tibial slope markedly increases ACL force in both active gait and passive knee joint under compression. J Biomech 47(6):1353–1359
Nagai K, Tashiro Y, Herbst E, Gale T, Wang JH, Irrgang JJ et al (2018) Steeper posterior tibial slope correlates with greater tibial tunnel widening after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 26(12):3717–3723
Ohori T, Mae T, Shino K, Tachibana Y, Yoshikawa H, Nakata K (2020) Tibial tunnel enlargement after anatomic anterior cruciate ligament reconstruction with a bone patellar tendon bone graft. Part 2: Factors related to the tibial tunnel enlargement. J Orthop Sci 25(2):279–284
Rahnemai-Azar AA, Yaseen Z, van Eck CF, Irrgang JJ, Fu FH, Musahl V (2016) Increased lateral tibial plateau slope predisposes male college football players to anterior cruciate ligament injury. J Bone Joint Surg Am 98(12):1001–1006
Sabat D, Kundu K, Arora S, Kumar V (2011) Tunnel widening after anterior cruciate ligament reconstruction: a prospective randomized computed tomography-based study comparing 2 different femoral fixation methods for hamstring graft. Arthroscopy 27(6):776–783
Sabzevari S, Rahnemai-Azar AA, Shaikh HS, Arner JW, Irrgang JJ, Fu FH (2017) Increased lateral tibial posterior slope is related to tibial tunnel widening after primary ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 25(12):3906–3913
Schneider CA, Rasband WS, Eliceiri KW (2012) NIH Image to ImageJ: 25 years of image analysis. Nat Methods 9(7):671–675
Segawa H, Omori G, Tomita S, Koga Y (2001) Bone tunnel enlargement after anterior cruciate ligament reconstruction using hamstring tendons. Knee Surg Sports Traumatol Arthrosc 9(4):206–210
Shino K, Nakata K, Nakamura N, Toritsuka Y, Horibe S, Nakagawa S, Suzuki T (2008) Rectangular tunnel double bundle anterior cruciate ligament reconstruction with bone patellar tendon-bone graft to mimic natural fiber arrangement. Arthroscopy 24(10):1178–1183
Shino K, Suzuki T, Iwahashi T, Mae T, Nakamura N, Nakata K, Nakagawa S (2010) The resident’s ridge as an arthroscopic landmark for anatomical femoral tunnel drilling in ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 18(9):1164–1168
Song GY, Zhang H, Wang QQ, Zhang J, Li Y, Feng H (2016) Risk factors associated with grade 3 pivot shift after acute anterior cruciate ligament injuries. Am J Sports Med 44(2):362–369
Taketomi S, Inui H, Yamagami R, Kawaguchi K, Nakazato K, Kono K et al (2020) Length of the tendon within the tibial tunnel affects tibial tunnel widening following anatomic anterior cruciate ligament reconstruction using a bone–patellar tendon–bone graft. J Knee Surg 33(5):445–451
Taketomi S, Inui H, Nakamura K, Yamagami R, Tahara K, Sanada T et al (2016) Secure fixation of femoral bone plug with a suspensory button in anatomical anterior cruciate ligament reconstruction with bone-patellar tendon bone graft. Joints 3(3):102–108
Taketomi S, Inui H, Tahara K, Shirakawa N, Tanaka S, Nakagawa T (2017) Effects of initial graft tension on femoral tunnel widening after anatomic anterior cruciate ligament reconstruction using a bone-patellar tendon-bone graft. Arch Orthop Trauma Surg 137(9):1285–1291
Taketomi S, Inui H, Sanada T, Yamagami R, Tanaka S, Nakagawa T (2014) Eccentric femoral tunnel widening in anatomic anterior cruciate ligament reconstruction. Arthroscopy 30(6):701–709
Taketomi S, Inui H, Yamagami R, Shirakawa N, Kawaguchi K, Nakagawa T, Tanaka S (2018) Bone-patellar tendon-bone autograft versus hamstring tendon autograft for anatomical anterior cruciate ligament reconstruction with three-dimensional validation of femoral and tibial tunnel positions. J Knee Surg 31(9):866–874
Tensho K, Shimodaira H, Aoki T, Narita N, Kato H, Kakegawa A et al (2014) Bony landmarks of the anterior cruciate ligament tibial footprint: a detailed analysis comparing 3-dimensional computed tomography images to visual and histological evaluations. Am J Sports Med 42(6):1433–1440
Siebold R, Schuhmacher P, Fernandez F, Śmigielski R, Fink C, Brehmer A, Kirsch J (2015) Flat midsubstance of the anterior cruciate ligament with tibial “C”-shaped insertion site. Knee Surg Sports Traumatol Arthrosc 23(11):3136–3142
Vasta S, Andrade R, Pereira R, Bastos R, Battaglia AG, Papalia R, Espregueira-Mendes J (2018) Bone morphology and morphometry of the lateral femoral condyle is a risk factor for ACL injury. Knee Surg Sports Traumatol Arthrosc 26(9):2817–2825
Weber AE, Delos D, Oltean HN, Vadasdi K, Cavanaugh J, Potter HG, Rodeo SA (2015) Tibial and femoral tunnel changes after ACL reconstruction: a prospective 2-year longitudinal MRI study. Am J Sports Med 43(5):1147–1156
Wilson TC, Kantaras A, Atay A, Johnson DL (2004) Tunnel enlargement after anterior cruciate ligament surgery. Am J Sports Med 32(2):543–549
Xu Y, Ao Y, Wang J, Yu J, Cui G (2011) Relation of tunnel enlargement and tunnel placement after single-bundle anterior cruciate ligament reconstruction. Arthroscopy 27(7):923–932
Yanagisawa S, Kimura M, Hagiwara K, Ogoshi A, Nakagawa T, Shiozawa H, Ohsawa T (2018) Patient age as a preoperative factor associated with tunnel enlargement following double-bundle anterior cruciate ligament reconstruction using hamstring tendon autografts. Knee Surg Sports Traumatol Arthrosc 26(4):1230–1236
Yoon KH, Park SY, Park JY, Kim EJ, Kim SJ, Kwon YB, Kim SG (2020) Influence of posterior tibial slope on clinical outcomes and survivorship after anterior cruciate ligament reconstruction using hamstring autografts: a minimum of 10-year follow-up. Arthroscopy 36(10):2718–2727
Ziegler CG, DePhillipo NN, Kennedy MI, Dekker TJ, Dornan GJ, LaPrade RF (2020) Beighton score, tibial slope, tibial subluxation, quadriceps circumference difference, and family history Are Risk factors for ACL graft failure: a retrospective comparison of primary and revision ACL reconstructions. Arthroscopy. https://doi.org/10.1016/j.arthro.2020.08.031
Funding
This study was no sources of funding.
Author information
Authors and Affiliations
Contributions
KN, ShT, RY and KK collected the data. ShT, HI and SaT designed the study. KN, ShT and HI analysed and interpreted the data. KN and ShT drafted the manuscript. All authors had complete access to all data (including statistical reports and tables) used in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Shuji Taketomi has received grants from Smith & Nephew outside this study. Shuji Taketomi has received a speaker honorarium from Smith & Nephew and Arthrex outside this study. No author has a conflict of interest regarding the topics discussed in this study.
Ethical approval
The institutional review board approved this retrospective study.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nakazato, K., Taketomi, S., Inui, H. et al. Lateral posterior tibial slope and length of the tendon within the tibial tunnel are independent factors to predict tibial tunnel widening following anatomic anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 29, 3818–3824 (2021). https://doi.org/10.1007/s00167-020-06419-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-020-06419-1