
Abstract
Aims/Hypothesis
The relationships between smoking and glycaemic variables have not been well explored. We compared HbA1c, fasting plasma glucose (FPG) and 2 h plasma glucose (2H-PG) in current, ex- and never-smokers.
Methods
This meta-analysis used individual data from 16,886 men and 18,539 women without known diabetes in 12 DETECT-2 consortium studies and in the French Data from an Epidemiological Study on the Insulin Resistance Syndrome (DESIR) and Telecom studies. Means of three glycaemic variables in current, ex- and never-smokers were modelled by linear regression, with study as a random factor. The I 2 statistic was used to evaluate heterogeneity among studies.
Results
HbA1c was 0.10% (95% CI 0.08, 0.12) (1.1 mmol/mol [0.9, 1.3]) higher in current smokers and 0.03% (0.01, 0.05) (0.3 mmol/mol [0.1, 0.5]) higher in ex-smokers, compared with never-smokers. For FPG, there was no significant difference between current and never-smokers (−0.004 mmol/l [−0.03, 0.02]) but FPG was higher in ex-smokers (0.12 mmol/l [0.09, 0.14]). In comparison with never-smokers, 2H-PG was lower (−0.44 mmol/l [−0.52, −0.37]) in current smokers, with no difference for ex-smokers (0.02 mmol/l [−0.06, 0.09]). There was a large and unexplained heterogeneity among studies, with I 2 always above 50%; I 2 was little changed after stratification by sex and adjustment for age and BMI. In this study population, current smokers had a prevalence of diabetes that was 1.30% higher as screened by HbA1c and 0.52% lower as screened by 2H-PG, in comparison with never-smokers.
Conclusion/interpretation
Across this heterogeneous group of studies, current smokers had a higher HbA1c and lower 2H-PG than never-smokers. This will affect the chances of smokers being diagnosed with diabetes.
Similar content being viewed by others

Introduction
The prevalence of type 2 diabetes is still increasing. Providing current and future estimates of diabetes prevalence is essential for public health planning. It is also important to be aware of factors associated with screen-detected diabetes to interpret these prevalences, and to provide appropriate prevention programmes. In this study we investigate smoking, a recognised risk factor for diabetes: a meta-analysis by Willi et al reported a pooled adjusted relative risk (95% CI) for incident diabetes of 1.44 (1.31, 1.58) for current smokers compared with non-smokers [1].
An individual’s phenotype and behavioural characteristics affect the chances of detecting diabetes by screening, according to whether fasting plasma glucose (FPG) or 2 h plasma glucose (2H-PG) following an OGTT is used [2, 3]; this appears to also be the case for HbA1c, in comparison with screen-detected diabetes using FPG or 2H-PG [4]. For participants in the Inter99 study who were screen-detected with diabetes by HbA1c (but not by OGTT results), fewer had hypertension or raised triacylglycerols, but more smoked in comparison with those detected by the OGTT results (but not by HbA1c) [4]. This latter result led us to further investigate the link between smoking and these three glycaemic variables.
The association between smoking status and the glycaemic variables HbA1c, FPG and 2H-PG has been studied, but few have studied all three variables in the same population. A higher HbA1c was found in smokers in six studies [5–10]; three studies showed no difference in FPG between smokers and non-smokers [9, 11, 12], while one study showed a lower FPG in smokers [13]; and 2H-PG was lower in smokers in two studies [9, 11] and higher in one study [12].
The aim of our study was to assess and quantify the influence of smoking status on mean values of HbA1c, FPG and 2H-PG in populations of adults worldwide, and so describe the potential impact of smoking in the context of screening for diabetes by one of these glycaemic variables.
Methods
Study population
The Evaluation of Screening and Early Detection Strategies for Type 2 Diabetes and Impaired Glucose Tolerance (DETECT-2) study aims to investigate the detection of type 2 diabetes using existing epidemiological studies around the world, with data on FPG and 2H-PG. In our analysis, we included 12 studies from the DETECT-2 consortium that also contained information on HbA1c and for which the principal investigator agreed to participate, as well as two additional French studies. The studies included from DETECT-2 were: the Australian Diabetes, Obesity and Lifestyle study (AusDiab), Australia [14]; Japanese–Brazilian Diabetes study, Brazil [15]; a population study in Qingdao, China [16]; The Inter99 study, Denmark [17]; Diabetes in Egypt Study, Egypt [18]; the Finnish cohort of the Seven Countries Study, Finland [19]; Chennai Urban Rural Epidemiology Study (CURES), India [20]; the Kenyan Diabetes Study, Kenya [21]; the Hoorn Study, the Netherlands [22]; a Tonga population-based study, Tonga [23]; the Seattle Japanese American Community Diabetes Study, from greater Seattle, USA [24]; and the National Health and Nutrition Examination Survey (NHANES III), USA [25]. The two additional French studies included in the analyses were the Data from an Epidemiological Study on the Insulin Resistance Syndrome (DESIR) study in a general population [26] and a study that enrolled employees from the Telecom Company in the Ile de France region [5]. All studies were approved by local ethics committees.
For the studies in Egypt and Kenya and in the French Telecom study, the questionnaires did not distinguish between ex- and never-smokers, and ex-smokers were therefore grouped with never-smokers to give two groups: current smokers and non-smokers. Data were not available on time since quitting smoking, making us unable to define ex-smokers precisely.
Assay methods for HbA1c and glucose are detailed in the Electronic Supplementary Material (ESM) Table 1.
The original data for participants from each study were available for analysis. We excluded participants with known diabetes and those with missing data on sex, age, BMI, smoking status, HbA1c, FPG or 2H-PG, with one exception: the DESIR study had no data on 2H-PG. The final study population included 16,886 men and 18,539 women (35,425 participants).
Statistical analyses
The populations studied are described by mean ± SD and n (%). The mean differences (95% CI) in HbA1c, FPG and 2H-PG for ex- and current smokers in comparison with never-smokers are presented, by study, in forest plots; all studies were combined, and the mean differences were evaluated using a mixed model, with study included as a random effect. The I 2 statistic was calculated to evaluate the heterogeneity between studies [27]. We tested for interactions between smoking status with sex and with age and BMI class on the entire study population. The differences in the glycaemic variables for ex- and current smokers in comparison with never-smokers are shown, stratified by these covariates, as some of the interactions were significant. Furthermore, we evaluated the sensitivity of the results by (1) stratifying by sex and adjusting for age and BMI; (2) restricting analyses to the seven studies from Western populations with similar exposures to smoking; (3) deleting the three studies that combined never- and ex-smokers; and (4) combining ex- and never-smokers in analyses.
From the pooled data, we estimated the prevalence of screened diabetes for never-, ex- and current smokers, as defined by the three criteria: HbA1c ≥6.5% (47.5 mmol/mol), FPG ≥7.0 mmol/l and 2H-PG ≥11.1 mmol/l. To quantify the effect of smoking on these prevalences, we calculated the mean differences between ex- and never-smokers and between current and never-smokers, for each of the three glycaemic variables. For ex- and current smokers, we then adjusted the participants’ values for the three glycaemic variables, by subtracting these mean differences, to estimate the values of the glycaemic variables had each individual been a never-smoker. Thus, the mean values of the glycaemic variables were adjusted so that they were equal for never-, ex- and non-smokers. As an example, the mean FPG among ex-smokers was 0.12 mmol/l higher than for never-smokers (ESM Table 2); 0.12 mmol/l was subtracted from the FPG value of each ex-smoker to give an adjusted FPG value, and diabetes prevalence was calculated on these adjusted FPG values.
SAS version 9.3 (Cary, NC, USA) was used in all statistical analyses.
Results
Characteristics differed significantly among cohorts (p < 0.0001): mean age varied between 37 ± 10 years (Kenyan women) and 76 ± 4 years (Finnish men) and the highest mean BMI was in Tongan women 35.2 ± 6.3 kg/m2. The means of glycaemic variables (HbA1c, FPG and 2H-PG) differed among cohorts: the highest mean HbA1c (6.4 ± 1.0% [46.4 ± 10.9 mol/mol]) was in Japanese–American men, and the highest mean FPG (7.7 ± 1.5 mmol/l) and 2H-PG (11.5 ± 5.1 mmol/l) were in Japanese–Brazilian men (Tables 1 and 2).
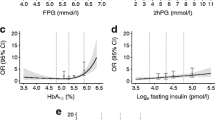
The mean HbA1c was higher in current compared with never-smokers in ten of the 14 studies and significantly higher in seven studies; in the Egyptian study, the mean HbA1c was 0.33% lower (significantly lower) in current smokers in comparison with never-smokers. In most studies, the mean HbA1c was not significantly different in never- and ex-smokers. Combining all studies, and adjusting for study as a random factor, HbA1c was 0.10% (95% CI 0.08, 0.12) (1.1 mmol/l [0.9, 1.3]) higher in current smokers and 0.03% (0.01, 0.05) (0.3 mmol/l [0.1, 0.5]) higher in ex-smokers compared with never-smokers (Fig. 1a, ESM Table 2). This relationship was consistent across sex, age and BMI strata for current smokers, but not among ex-smokers (Table 3).

(a) The difference in mean (95% CI) HbA1c between current smokers and never-smokers was 0.10% (0.08, 0.12) (1.1 mmol/mol [0.9, 1.3]); between ex-smokers and never-smokers it was 0.03% (0.01, 0.05) (0.3 mmol/mol [0.1, 0.5]). The I 2 heterogeneity statistic was 93% and 55%, respectively. To convert values for HbA1c in % into mmol/mol, subtract 2.15 and multiply by 10.929 or use the conversion calculator at www.HbA1c.nu/eng. (b) The difference in mean (95% CI) FPG between current smokers and never-smokers was −0.004 mmol/l (−0.06, 0.02); between ex-smokers and never-smokers it was 0.12 mmol/l (0.09, 0.14). The I 2 heterogeneity statistic was 71% and 89%, respectively. (c) The difference in mean (95% CI) 2H-PG between current smokers and never-smokers was −0.44 mmol/l (−0.52, −0.37); between ex-smokers and never-smokers it was 0.02 mmol/l (−0.06, 0.09). The I 2 heterogeneity statistic was 88% and 62%, respectively. France-T, French Telecom study; France-D, French DESIR study; USA-J, US Japanese-American study; USA-N, US NHANES study
In the study of Japanese–Brazilians, the mean FPG was significantly higher by 0.66 mmol/l in current smokers than in never-smokers, and in the Egyptian and French Telecom studies it was significantly lower by 0.55 and 0.06 mmol/l, respectively. However, in all other studies, the mean FPG did not differ between current and never-smokers (Fig. 1b, ESM Table 2). Combining studies, there was no significant difference in FPG between current and never-smokers; ex-smokers had a 0.12 mmol/l (0.09, 0.14) higher FPG than never-smokers, and this relationship was seen in all three age and BMI strata, and was consistent across age and BMI classes (Table 3).
The mean 2H-PG of current smokers was lower than that of never-smokers in all studies, except for the Indian CURES study. When the studies were combined, 2H-PG in current smokers was lower by −0.44 mmol/l (−0.52, −0.37) in comparison with never-smokers (Fig. 1c, ESM Table 2). These relations were consistent over sex, age and BMI strata (Table 3). In contrast, 2H-PG did not differ among ex-smokers and never-smokers.
When we stratified by sex, and adjusted for age and BMI, the differences in the glycaemic variables between current and never-smokers were consistent with the unadjusted differences, and were also consistent in the seven studies from ‘Western’ populations (ESM Table 2). The comparisons between ex- and never-smokers were less consistent (ESM Table 2).
As might be expected from Fig. 1, we found heterogeneity among studies, with an I 2 of 93% for differences in mean HbA1c for current smokers and 55% for ex-smokers in comparison with never-smokers; for FPG, I 2 was 71% for current smokers and 89% for ex-smokers; for 2H-PG, I 2 was 88% for current smokers and 62% for ex-smokers. We stratified by sex and adjusted for age and BMI to determine whether the resulting heterogeneity would be reduced (ESM Fig. 1–3). This was the case for some of the comparisons; for ex-smokers, the within-study heterogeneity was high in comparison with the between-study heterogeneity (ESM Table 3), but there were still some I 2 values of more than 90%.
In a sensitivity analysis, we excluded the three studies where ex- and never-smokers were combined, but there was still high heterogeneity among studies. Furthermore, when we combined never- and ex-smokers as non-smokers, current smokers compared with non-smokers had a significantly higher HbA1c (0.09% [95% CI 0.07, 0.11]) (1.0 mmol/mol [0.8, 1.2]) but significantly lower FPG (−0.04 mmol/l [−0.06, −0.01]) and 2H-PG (−0.45 mmol/l [−0.51, −0.40]).
As sex, age and BMI are correlated with the three glycaemic variables, we tested the interactions among smoking status and strata of these variables. Interactions with sex were significant, but those with age and BMI strata were not significant except for the relationship of smoking with age for HbA1c (Table 3).
Comparing current smokers with never-smokers, HbA1c showed a significantly greater difference in men than in women, at 0.13% (95% CI 0.11, 0.15) and 0.05% (0.02, 0.07) (1.4 mmol/mol [1.2, 1.6] and 0.5 mmol/mol [0.2, 0.8]), respectively (Table 3). In contrast, while men who were ex-smokers had a higher HbA1c than never-smokers, women had a lower HbA1c. For the three age strata, the differences were all significant comparing current and never-smokers; the differences were all positive but smaller for ex-smokers. For the three BMI strata, the HbA1c differences were very similar for both current and ex-smokers.
When FPG was analysed according to strata, it was mainly ex-smokers for whom the FPG was significantly higher than for never-smokers; for current smokers, women had a significantly lower FPG.
For 2H-PG and current smokers, all strata had significantly lower values than never-smokers. For ex-smokers, the only significant difference was for sex (Table 3), and these results paralleled those for HbA1c: for ex-smokers, men had a higher and women had a lower 2H-PG than never-smokers.
For the population included in this study, we show the prevalences of screened diabetes according to each of the three glycaemic variables (Table 4), using the original crude data and then the adjusted prevalences for ex- and current smokers, after subtracting constants from the concentrations for ex- and current smokers, so that the mean values were identical to those of never-smokers. In current smokers, the prevalence of diabetes screened by HbA1c changed from 5.32% to 4.02%, a 1.30% lower prevalence of diabetes after this adjustment; there was no change for FPG; for 2H-PG the crude prevalence was 3.36% and the adjusted prevalence was 3.88%; thus, the prevalence was 0.52% higher after adjustment. For ex-smokers, all prevalences were increased after adjustment: by 0.71% for HbA1c, by 0.82% for FPG and by 0.16% for 2H-PG.
Discussion
Compared with never-smokers, current smokers had a 0.10% (1.1 mmol/mol) higher HbA1c, no difference in FPG and 0.44 mmol/l lower 2H-PG. These results remained consistent when never- and ex-smokers were combined. In most of the individual studies in our analyses, the mean HbA1c was significantly higher in current smokers than in never-smokers; for FPG, the difference between smokers and never-smokers was not significant in 11 of the 14 studies and for 2H-PG, the means were significantly lower in current smokers than in never-smokers in nine of the 14 studies. The differences in mean HbA1c, FPG and 2H-PG between never- and ex-smokers were not significant in about half of the studies.
One of the strengths of our work is the large number of participants from 14 studies from countries around the world. However, there will be measurement error in both the exposure to smoking and in the glycaemic outcome measures (HbA1c, FPG and 2H-PG) within and across these studies.
One of the limitations of our study is the high heterogeneity across studies, with I 2 statistics, which measure the difference between individual studies, being greater than 50% for the three variables (HbA1c, FPG and 2H-PG) for both current smokers and ex-smokers. The heterogeneity statistic I 2 was lower for some variables after stratifying for sex and adjusting for age and BMI, but remained high for others; similar results were obtained when analyses were restricted to the more comparable Western populations, and when those studies that combined ex- and never-smokers were not included in analyses. Indeed, the larger studies added greatly to the I 2 measure. As we studied mean differences in the glycaemic measures across smoking-status groups for each study, measurement error in the outcomes (differences of means) across studies because of different normal values of the assays is less likely to be a reason for high heterogeneity. There will be measurement error for smoking status, as reported in questionnaires, and as perceived by the participants who answered the questions on smoking.
Furthermore, tobacco consumption was not coded in the same way for all studies: in the French Telecom study, those who had been ex-smokers for less than 6 months were considered to be current smokers and only those who had stopped smoking for more than 6 months were considered non-smokers; in the studies from Kenya and Egypt, ex-smokers were not coded. While the definition of never-smokers might be unambiguous, the time since ex-smokers had quit smoking might differ between studies.
There were also some differences in the outcome measures among studies. In Tonga, the OGTT was only performed in participants with fasting capillary glucose between 5.0 and 11.1 mmol/l or with fasting capillary glucose ≤5 mmol/l and HbA1c >6.0% (42.1 mmol/mol), as well as in one in five participants with fasting glucose ≤5 mmol/l [23]. Mean HbA1c differed among studies, more than that of glucose, as we have shown in other analyses [28, 29]. Indeed, in the study of Japanese–Americans [24], the mean HbA1c was much higher than in other studies. HbA1c was assayed over a long time period, and the techniques used were certainly not aligned with the recent International Federation of Clinical Chemistry standard [30], although the assays for some studies were aligned with the National Glycohemoglobin Standardization Program that was used for the DCCT and the UK Prospective Diabetes Study [31, 32]. However, as commented above, for the main analyses shown on the forest plots, we are dealing with differences within centres in comparison with never-smokers.
Finally, adding to the heterogeneity within and among studies were differences in ethnicity, socioeconomic levels, dietary habits and characteristics of participants—for example, age and BMI.
Studies that have previously examined these glycaemic measurements as a function of tobacco consumption have, in the main, found similar results to ours, despite being analysed differently and adjusted for different factors.
In the meta-analysis by Willi et al [1], smoking was convincingly shown to be associated with an increased risk of developing type 2 diabetes, even after taking into account different confounding factors and despite the fact that diabetes was not defined homogeneously over studies; however, a causal relation cannot be assumed. Various authors have hypothesised mechanisms that might generate changes in glucose metabolism, leading to diabetes [32, 33]. Several studies have shown that smoking reduces insulin sensitivity [33, 34], and this may be due to nicotine as it stimulates the secretion of insulin-antagonising hormones such as cortisol, catecholamines and growth hormone, which impair the action of insulin [33]. However Wareham et al concluded that a causal relationship is unlikely [11], as the relationship was attenuated after adjusting for age and BMI. Alterations in insulin secretion have not been shown to be associated with smoking [33]. It is also probable that smokers have other unhealthy behaviours and dietary habits as well as a low socioeconomic status, and these are well-recognised risk factors for diabetes [1].
It is of note that we (and others) have found associations between smoking and HbA1c and 2H-PG in opposing directions. One can speculate that HbA1c assay techniques might be affected by a metabolite of tobacco. A study in smokers and non-smokers using the International Federation of Clinical Chemistry reference assay, which analyses only one molecular species of glycated A1c, would confirm or refute this hypothesis. Higgins et al have hypothesised that smoking might induce increased permeability of the erythrocyte membrane to the passage of glucose, thus increasing HbA1c [35]. Smoking has been associated with both lower arterial oxygen saturation and higher erythrocyte 2,3-diphosphorglycerate concentrations. In vitro studies have demonstrated that deoxyhaemoglobin is glycated more rapidly than oxyhaemoglobin [36], and the rate of HbA1c formation is increased with elevated 2,3-diphosphorglycerate concentrations. Another possibility is the effect of tobacco smoking on erythrocyte lifespan. Carbon monoxide, administered to two patients with sickle-cell disease, was found to increase erythrocyte lifespan [37]. Further studies are needed to assess the role of these factors.
Some authors have reported that smoking inhibits gastric motor activity [38, 39] and may therefore affect the rate at which a meal (or the glucose in an OGTT) is absorbed. Other authors have studied the effect of tobacco on solid and liquid meals separately, and found that cigarette smoking accelerates the emptying of the liquid component of meals [40]. In agreement with this report, Janzon et al showed a dose–response relationship between glucose and habitual cigarette consumption at 40 min following an OGTT, and the inverse relationship at 120 min, indicating a quicker absorption of glucose [41]. This was corroborated in the EGIR-RISC STUDY [42]: age-, sex- and BMI-adjusted glucose concentrations were identical at fasting in current and never-smokers, significantly higher in current smokers at 30 and 60 min, no difference between the two groups at 90 min and significantly lower in current smokers at 120 min (B. Balkau, unpublished data); smokers therefore appear to have accelerated gastric emptying during an OGTT. Furthermore, the area under the glucose curve during the OGTT was significantly higher in current smokers, and this would presumably lead to a higher HbA1c.
Overall in our study population, using data from our study, screening for diabetes using HbA1c, rather than the formerly considered gold standard of 2H-PG, would result in a 1.8% higher prevalence of diabetes in current smokers, due to the higher HbA1c and lower 2H-PG levels in current smokers. Using HbA1c as a screening test should have the beneficial effect of preferentially identifying current smokers with high HbA1c, and so provide the possibility for early preventive measures with an encouragement to stop smoking. For ex-smokers, both HbA1c and 2H-PG levels were higher than in never-smokers, with a net difference of 0.55% in prevalence.
In conclusion, previous publications have shown that smoking is associated with an increased risk of diabetes. In our meta-analysis, we found that HbA1c levels were higher in smokers than in non-smokers; this was not the case for FPG and indeed 2H-PG levels were lower. The mechanisms explaining the higher level of HbA1c and the lower level of 2H-PG in smokers need to be further explored.
Abbreviations
- CURES:
-
Chennai Urban Rural Epidemiology Study
- DESIR:
-
Data from an Epidemiological Study on the Insulin Resistance Syndrome
- FPG:
-
Fasting plasma glucose
- 2H-PG:
-
2 h Plasma glucose
References
Willi C, Bodenmann P, Ghali WA, Faris PD, Cornuz J (2007) Active smoking and the risk of type 2 diabetes: a systematic review and meta-analysis. JAMA 298:2654–2664
Sicree RA, Zimmet PZ, Dunstan DW, Cameron AJ, Welborn TA, Shaw JE (1988) Differences in height explain gender differences in the response to the oral glucose tolerance test—the AusDiab study. Diabet Med 25:296–302
DECODE Study Group on behalf of the European Diabetes Epidemiology Study Group (1998) Will new diagnostic criteria for diabetes mellitus change phenotype of patients with diabetes? Reanalysis of European epidemiological data. BMJ 317:371–375
Borg R, Vistisen D, Witte DR, Borch-Johnsen K (2010) Comparing risk profiles of individuals diagnosed with diabetes by OGTT and HbA1c. The Danish Inter99 study. Diabet Med 27:906–910
Simon D, Senan C, Garnier P, Saint-Paul M, Papoz L (1989) Epidemiological features of glycated haemoglobin A1c-distribution in a healthy population. The Telecom Study. Diabetologia 32:864–869
Yudkin JS, Forrest RD, Jackson CA, Ryle AJ, Davie S, Gould BJ (1990) Unexplained variability of glycated haemoglobin in non-diabetic subjects not related to glycaemia. Diabetologia 33:208–215
Nilsson PM, Lind L, Pollare T, Berne C, Lithell HO (1995) Increased level of hemoglobin A1C but not impaired insulin sensitivity, found in hypertensive and normotensive smokers. Metabolism 44:557–561
Sargeant LA, Khaw KT, Bingham S et al (2001) Cigarette smoking and glycaemia: the EPIC-Norfolk Study. European Prospective Investigation into Cancer. Int J Epidemiol 30:547–554
Cho NH, Chan JC, Jang HC, Lim S, Kim HL, Choi SH (2009) Cigarette smoking is an independent risk factor for type 2 diabetes: a four-year community-based prospective study. Clin Endocrinol (Oxf) 71:679–685
Clair C, Bitton A, Meigs JB, Rigotti NA (2011) Relationships of cotinine and self-reported cigarette smoking with hemoglobin A1c in the U.S.: results from the National Health and Nutrition Examination Survey, 1999-2008. Diabetes Care 34:2250–2255
Wareham NJ, Ness EM, Byrne CD, Cox BD, Day NE, Hales CN (1996) Cigarette smoking is not associated with hyperinsulinemia: evidence against a causal relationship between smoking and insulin resistance. Metabolism 45:1551–1556
Frati AC, Iniestra F, Ariza CR (1996) Acute effect of cigarette smoking on glucose tolerance and other cardiovascular risk factors. Diabetes Care 19:112–118
Masulli M, Riccardi G, Galasso R, Vaccaro O (2006) Relationship between smoking habits and the features of the metabolic syndrome in a non-diabetic population. Nutr Metab Cardiovasc Dis 16:364–370
Dunstan DW, Zimmet PZ, Welborn TA et al (2002) The Australian Diabetes, Obesity and Lifestyle Study (AusDiab)—methods and response rates. Diabetes Res Clin Pract 57:119–129
Gimeno SG, Ferreira SR, Franco LJ, Hirai AT, Matsumura L, Moises RS (2002) Prevalence and 7-year incidence of type II diabetes mellitus in a Japanese-Brazilian population: an alarming public health problem. Diabetologia 45:1635–1638
Zhou X, Pang Z, Gao W et al (2011) Fresh vegetable intake and prevalence of diabetes in a Chinese population in Qingdao. Diabetes Res Clin Pract 92:137–142
Glumer C, Jorgensen T, Borch-Johnsen K (2003) Prevalences of diabetes and impaired glucose regulation in a Danish population: the Inter99 study. Diabetes Care 26:2335–2340
Herman WH, Ali MA, Aubert RE et al (1995) Diabetes mellitus in Egypt: risk factors and prevalence. Diabet Med 12:1126–1131
Stengard JH, Tuomilehto J, Pekkanen J et al (1992) Diabetes mellitus, impaired glucose tolerance and mortality among elderly men: the Finnish cohorts of the Seven Countries Study. Diabetologia 35:760–765
Deepa M, Pradeepa R, Rema M et al (2003) The Chennai Urban Rural Epidemiology Study (CURES)—study design and methodology (urban component) (CURES-I). J Assoc Physicians India 51:863–870
Christensen DL, Friis H, Mwaniki DL et al (2009) Prevalence of glucose intolerance and associated risk factors in rural and urban populations of different ethnic groups in Kenya. Diabetes Res Clin Pract 84:303–310
de Vegt F, Dekker JM, Ruhe HG et al (1999) Hyperglycaemia is associated with all-cause and cardiovascular mortality in the Hoorn population: the Hoorn Study. Diabetologia 42:926–931
Colagiuri S, Colagiuri R, Na’ati S, Muimuiheata S, Hussain Z, Palu T (2002) The prevalence of diabetes in the Kingdom of Tonga. Diabetes Care 25:1378–1383
Fugimoto W, Boyko EJ, Leonetti DL, Bergstrom R, Newell-Morris L, Wahl PW (1996) Hypertension in Japanese Americans: the Seattle Japanese-American Community Study. Public Health Rep III (Suppl 2):S56–S58
Alexander CM, Landsman PB, Teutsch SM, Haffner SM (2003) NCEP-defined metabolic syndrome, diabetes, and prevalence of coronary heart disease among NHANES III participants age 50 years and older. Diabetes 52:1210–1214
Balkau B, Lange C, Fezeu L et al (2008) Predicting diabetes: clinical, biological, and genetic approaches: data from the Epidemiological Study on the Insulin Resistance Syndrome (DESIR). Diabetes Care 31:2056–2061
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analysis. BMJ 327:557–560
Soulimane S, Simon D, Shaw JE et al (2011) Comparing incident diabetes as defined by fasting plasma glucose or by HbA(1c). The AusDiab, Inter99 and DESIR studies. Diabet Med 28:1311–1318
Soulimane S, Simon D, Shaw J et al (2012) HbA1c, fasting plasma glucose and the prediction of diabetes: Inter99, AusDiab and D.E.S.I.R. Diabetes Res Clin Pract 96:392–399
Consensus Committee (2007) Consensus statement on the worldwide standardization of the hemoglobin A1C measurement: the American Diabetes Association, European Association for the Study of Diabetes, International Federation of Clinical Chemistry and Laboratory Medicine, and the International Diabetes Federation. Diabetes Care 30:2399–2400
The Diabetes Control and Complications Trial Research Group (1993) The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 329:977–986
Manley S (2003) Haemoglobin A1c—a marker for complications of type 2 diabetes: the experience from the UK Prospective Diabetes Study (UKPDS). Clin Chem Lab Med 41:1182–1190
Eliasson B (2003) Cigarette smoking and diabetes. Prog Cardiovasc Dis 45:405–413
Facchini FS, Hollenbeck CB, Jeppesen J, Chen YD, Reaven GM (1992) Insulin resistance and cigarette smoking. Lancet 339:1128–1130
Higgins T, Cembrowski G, Tran D, Lim E, Chan J (2009) Influence of variables on hemoglobin A1c values and nonheterogeneity of hemoglobin A1c reference ranges. J Diabetes Sci Technol 3:644–648
Smith RJ, Koenig RJ, Binnerts A, Soeldner JS, Aoki TT (1982) Regulation of hemoglobin AIc formation in human erythrocytes in vitro. Effects of physiologic factors other than glucose. J Clin Invest 69:1164–1168
Beutler E (1975) The effect of carbon monoxide on red cell life span in sickle cell disease. Blood 46:253–259
Kohagen KR, Kim MS, McDonnell WM, Chey WD, Owyang C, Hasler WL (1996) Nicotine effects on prostaglandin-dependent gastric slow wave rhythmicity and antral motility in nonsmokers and smokers. Gastroenterology 110:3–11
Johnson RD, Horowitz M, Maddox AF, Wishart JM, Shearman DJ (1991) Cigarette smoking and rate of gastric emptying: effect on alcohol absorption. BMJ 302:20–23
Grimes DS, Goddard J (1978) Effect of cigarette smoking on gastric emptying. BMJ 2:460–461
Janzon L, Berntorp K, Hanson M, Lindell SE, Trell E (1983) Glucose tolerance and smoking: a population study of oral and intravenous glucose tolerance tests in middle-aged men. Diabetologia 25:86–88
Hills SA, Balkau B, Coppack SW et al (2004) The EGIR-RISC STUDY (The European group for the study of insulin resistance: relationship between insulin sensitivity and cardiovascular disease risk): I. Methodology and objectives. Diabetologia 47:566–570
Acknowledgements
The DETECT-2 project was undertaken on the initiative of the World Health Organization and the International Diabetes Federation. DETECT-2: Task Group. Stephen Colagiuri and Crystal M. Y. Lee (Australia), Knut Borch-Johnsen and Dorte Vistisen (Denmark), Beverley Balkau (France), Jacqueline M. Dekker (the Netherlands). Crystal M. Y. Lee was supported by an Australian National Health and Medical Research Council Training Fellowship. Soraya Soulimane was supported by a PhD grant from Paris-Sud University, France. Jonathan E. Shaw was supported by an Australian National Health and Medical Research Council Senior Research Fellowship. Dirk L. Christensen was supported by a DANIDA grant and by a grant from the Cluster of International Health, University of Copenhagen.
Duality of interest
DV is employed by Steno Diabetes Center A/S, a research hospital working in the Danish National Health Service and owned by Novo Nordisk A/S. DV and KB-J own shares in Novo Nordisk A/S. The other authors declare no duality of interest.
Contribution statement
DV and BB conceived this study; SS and BB analysed and interpreted the data; SS and BB drafted the article. Authors DS, CL, WHH, SC, JES, PZZ, DM, SRGF, YD, LZ, TJ, JT, VM, DLC, LK, JMD, GN, CDAS, OL, WYF, DLL, MJMcN, KB-J, EJB, DV, BB conceived and designed their original individual studies and contributed to the data collection in their individual studies; CMYL and DV were responsible for co-ordinating the data in the DETECT-2 Study. All authors critically reviewed various drafts of the manuscript and all authors approved the final version.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Details of the DETECT-2 and DESIR study groups and their principal investigators are given in the electronic supplementary material (ESM).
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM Study Group Investigators
(PDF 90 kb)
ESM Fig. 1
(PDF 57 kb)
ESM Fig. 2
(PDF 51 kb)
ESM Fig. 3
(PDF 51 kb)
ESM Table 1
(PDF 12 kb)
ESM Table 2
(PDF 19 kb)
ESM Table 3
(PDF 13 kb)
Rights and permissions
About this article
Cite this article
Soulimane, S., Simon, D., Herman, W.H. et al. HbA1c, fasting and 2 h plasma glucose in current, ex- and never-smokers: a meta-analysis. Diabetologia 57, 30–39 (2014). https://doi.org/10.1007/s00125-013-3058-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-013-3058-y