
Abstract
Purpose
Patients without evidence of disease at radical cystectomy (RC) following neoadjuvant chemotherapy (NAC) have the greatest potential for survival in muscle-invasive bladder cancer. Historically, 15 % of such patients will experience disease recurrence and cancer-specific mortality. We sought to evaluate the effect of pre-treatment clinical factors on the risk of recurrence in patients who were ypT0N0 at RC.
Methods
We performed a multi-institutional review of patients treated with NAC + RC for muscle-invasive bladder cancer (≥cT2) without pathologic evidence of disease at surgery (ypT0N0). The association of pre-treatment clinicopathologic features with recurrence was evaluated using Cox proportional hazards.
Results
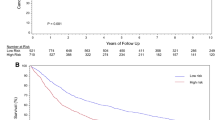
A total of 78 patients were identified with ypT0 disease at RC after NAC. Median postoperative follow-up was 32.4 months (IQR 16.8, 60.0), during which time 17 patients recurred at a median of 6.4 months after RC. Estimated 3-year recurrence-free survival (RFS) of this cohort was 74.8 %. In univariate analysis, cT4 disease (HR 3.12; p = 0.04) and time to RC (HR 1.17 for each month increase; p < 0.01) were associated with inferior RFS.
Conclusion
Patients without evidence of disease at the time of RC are still at risk of recurrence and death from bladder cancer. Higher clinical stage and increased time to RC were associated with an increased risk of recurrence and subsequent death. These data highlight the importance of timely RC and the continued risk of recurrence in higher clinically staged patients—underscoring the need for close monitoring and patient counseling.


Similar content being viewed by others


References
Siegel R et al (2014) Cancer statistics, 2014. CA Cancer J Clin 64(1):9–29
Grossman HB et al (2003) Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 349(9):859–866
Advanced Bladder Cancer Meta-analysis Collaboration (2005) Neoadjuvant chemotherapy in invasive bladder cancer: update of a systematic review and meta-analysis of individual patient data advanced bladder cancer (ABC) meta-analysis collaboration. Eur Urol 48(2):202–205 (discussion 205–206)
Rosenblatt R et al (2012) Pathologic downstaging is a surrogate marker for efficacy and increased survival following neoadjuvant chemotherapy and radical cystectomy for muscle-invasive urothelial bladder cancer. Eur Urol 61(6):1229–1238
Kassouf W et al (2007) P0 stage at radical cystectomy for bladder cancer is associated with improved outcome independent of traditional clinical risk factors. Eur Urol 52(3):769–774
Lavery HJ et al (2014) Pathological T0 following radical cystectomy with or without neoadjuvant chemotherapy: a useful surrogate. J Urol 191(4):898–906
Petrelli F et al (2014) Correlation of pathologic complete response with survival after neoadjuvant chemotherapy in bladder cancer treated with cystectomy: a meta-analysis. Eur Urol 65(2):350–357
Zargar H et al (2015) Multicenter assessment of neoadjuvant chemotherapy for muscle-invasive bladder cancer. Eur Urol 67(2):241–249
Edge SB, Compton CC (2010) The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 17(6):1471–1474
Zehnder P et al (2011) Super extended versus extended pelvic lymph node dissection in patients undergoing radical cystectomy for bladder cancer: a comparative study. J Urol 186(4):1261–1268
Clark PE et al (2013) Bladder cancer. J Natl Compr Canc Netw 11(4):446–475
James AC et al (2014) Role of maximal endoscopic resection before cystectomy for invasive urothelial bladder cancer. Clin Genitourin Cancer 12(4):287–291
Meyer A et al (2014) The natural history of clinically complete responders to neoadjuvant chemotherapy for urothelial carcinoma of the bladder. J Urol 192(3):696–701
Svatek RS et al (2011) Discrepancy between clinical and pathological stage: external validation of the impact on prognosis in an international radical cystectomy cohort. BJU Int 107(6):898–904
Ploeg M et al (2012) Discrepancy between clinical staging through bimanual palpation and pathological staging after cystectomy. Urol Oncol 30(3):247–251
Gray PJ et al (2014) Clinical-pathologic stage discrepancy in bladder cancer patients treated with radical cystectomy: results from the national cancer data base. Int J Radiat Oncol Biol Phys 88(5):1048–1056
Tritschler S et al (2012) Staging of muscle-invasive bladder cancer: can computerized tomography help us to decide on local treatment? World J Urol 30(6):827–831
Papalia R et al (2012) Diffusion-weighted magnetic resonance imaging in patients selected for radical cystectomy: detection rate of pelvic lymph node metastases. BJU Int 109(7):1031–1036
Rouanne M et al (2014) Potential impact of 18F-FDG PET/CT on patients selection for neoadjuvant chemotherapy before radical cystectomy. Eur J Surg Oncol 40(12):1724–1730
Ozturk H (2015) Detecting metastatic bladder cancer using 18F-fluorodeoxyglucose positron-emission tomography/computed tomography. Cancer Res Treat 47(4):834–843
Maurer T et al (2012) Diagnostic efficacy of [11C] choline positron emission tomography/computed tomography compared with conventional computed tomography in lymph node staging of patients with bladder cancer prior to radical cystectomy. Eur Urol 61(5):1031–1038
Graziani T et al (2015) 11C-choline PET/CT for restaging of bladder cancer. Clin Nucl Med 40(1):e1–e5
Gore JL et al (2009) Mortality increases when radical cystectomy is delayed more than 12 weeks: results from a surveillance, epidemiology, and end results-medicare analysis. Cancer 115(5):988–996
Sonpavde G et al (2011) Disease-free survival at 2 or 3 years correlates with 5-year overall survival of patients undergoing radical cystectomy for muscle invasive bladder cancer. J Urol 185(2):456–461
Author contribution
Parker WP was involved in protocol development, data collection, data analysis and wrote the manuscript. Ho PL was involved in data collection and edited the manuscript. Boorjian SA, Holzbeierlein JM, Kamat AM and Lee EK were involved in protocol development and edited the manuscript. Melquist JJ was involved in data collection and edited the manuscript. Thapa P was involved in data collection, data analysis and edited the manuscript. Frank I edited the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Ashish M Kamat, MD has the following disclosures: Research Funding—FKD, Heat Biologics, Photocure, Telesta Therapeutics, Merk Abott Molecular, and Pacific Edge. Consulting—Sanofi, Taris, Telesta Therapeutics, Spectrum Pharmaceuticals, Theralase, MDX Health, Merck, Abbott Molecular, Heat Biologics, and Photocure. Advisory Board—Sanofi and Theralase. The authors declare that no other potential conflicts of interest exist.
Ethical statements
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Parker, W.P., Ho, P.L., Boorjian, S.A. et al. The importance of clinical stage among patients with a complete pathologic response at radical cystectomy after neoadjuvant chemotherapy. World J Urol 34, 1561–1566 (2016). https://doi.org/10.1007/s00345-016-1801-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-016-1801-y